Failed First Craniotomy and Tumor Removal of Parasagittal Meningioma with Severe Peritumoral Brain Edema
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University College of Medicine, Seoul, Korea. nslee@snu.ac.kr
- 2Department of Neurosurgery, SMG-Seoul National University Boramae Medical Center, Seoul, Korea.
- KMID: 2356981
- DOI: http://doi.org/10.14791/btrt.2016.4.2.124
Abstract
- Parasagittal meningioma often presents as peritumoral brain edema (PTBE). The risk of edema increases when the tumor occludes the superior sagittal sinus (SSS). Although PTBE may be expected based on the patient's symptoms or radiologic findings, extensive brain swelling and extracranial herniation during elective surgery are rare. Herniation during surgery could lead to irreversible neurological damage and even brain rupture. We report a case of a failed routine craniotomy for a parasagittal meningioma with complete occlusion of the posterior third of the SSS in a 30-year-old male patient. The patient developed extensive brain swelling and extracranial herniation during surgery.
Keyword
MeSH Terms
Figure
-
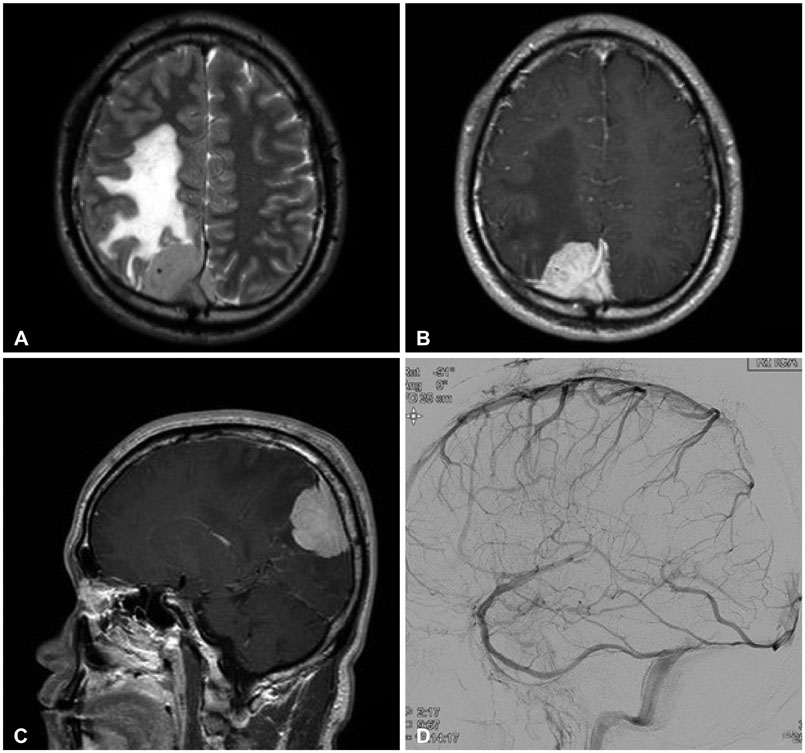
Fig. 1 Preoperative magnetic resonance imaging and cerebral angiographic findings. T2-weighted axial image shows dural-based iso-signal intensity mass in the parietal convexity along the superior sagittal sinus (SSS) with extensive perilesional edema (A); gadolinium-enhanced axial and sagittal image shows homogenous enhancement pattern (B and C); and right internal carotid angiography shows total occlusion of posterior third of the SSS (D).

Fig. 2 Transdural observation of the cortical arteries, veins, and venous sinus was performed using indocyanine green (ICG) videography. Visualization of the dural attachment of meningioma enabled safe and appropriate dural opening, minimizing damage to the venous channels. General microscopic findings (A) and ICG videographic findings (B). The black open arrows mark the tumor margin, and the white closed arrows mark the right lateral border of posterior third of the superior sagittal sinus.
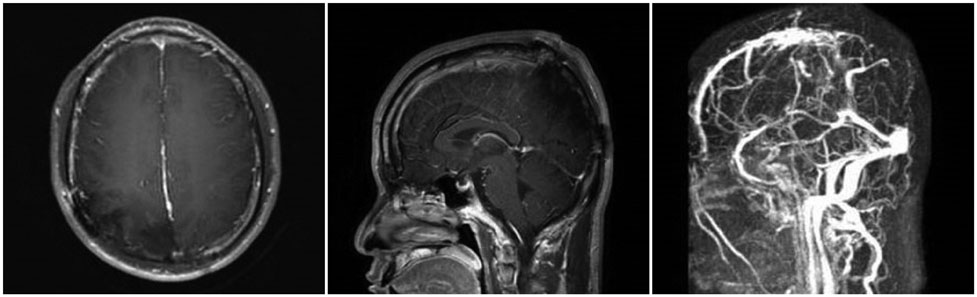
Fig. 3 Postoperative magnetic resonance imaging and venographic findings. Venography shows no residual enhancing mass and intact anterior superior sagittal sinus and other sinus drainage (straight, transverse, and sigmoid sinuses).
Reference
-
1. Abe T, Black PM, Ojemann RG, Hedley-White ET. Cerebral edema in intracranial meningiomas: evidence for local and diffuse patterns and factors associated with its occurrence. Surg Neurol. 1994; 42:471–475.
Article2. Challa VR, Moody DM, Marshall RB, Kelly DL Jr. The vascular component in meningiomas associated with severe cerebral edema. Neurosurgery. 1980; 7:363–368.
Article3. Go KG, Wilmink JT, Molenaar WM. Peritumoral brain edema associated with meningiomas. Neurosurgery. 1988; 23:175–179.
Article4. Inamura T, Nishio S, Takeshita I, Fujiwara S, Fukui M. Peritumoral brain edema in meningiomas--influence of vascular supply on its development. Neurosurgery. 1992; 31:179–185.
Article5. Whittle IR, Viswanathan R. Acute intraoperative brain herniation during elective neurosurgery: pathophysiology and management considerations. J Neurol Neurosurg Psychiatry. 1996; 61:584–590.
Article6. Sindou M, Auque J, Jouanneau E. Neurosurgery and the intracranial venous system. Acta Neurochir Suppl. 2005; 94:167–175.
Article7. Mantovani A, Di Maio S, Ferreira MJ, Sekhar LN. Management of meningiomas invading the major dural venous sinuses: operative technique, results, and potential benefit for higher grade tumors. World Neurosurg. 2014; 82:455–467.
Article8. Oh IH, Park BJ, Choi SK, Lim YJ. Transient neurologic deterioration after total removal of parasagittal meningioma including completely occluding superior sagittal sinus. J Korean Neurosurg Soc. 2009; 46:71–73.
Article9. Ojemann RG. Management of cranial and spinal meningiomas (honored guest presentation). Clin Neurosurg. 1993; 40:321–383.10. Stevens JM, Ruiz JS, Kendall BE. Observations on peritumoral oedema in meningioma. Part II: mechanisms of oedema production. Neuroradiology. 1983; 25:125–131.11. Yoshioka H, Hama S, Taniguchi E, Sugiyama K, Arita K, Kurisu K. Peritumoral brain edema associated with meningioma: influence of vascular endothelial growth factor expression and vascular blood supply. Cancer. 1999; 85:936–944.12. Osawa T, Tosaka M, Nagaishi M, Yoshimoto Y. Factors affecting peritumoral brain edema in meningioma: special histological subtypes with prominently extensive edema. J Neurooncol. 2013; 111:49–57.
Article13. Roth C, Ferbert A, Deinsberger W, et al. Does prone positioning increase intracranial pressure? A retrospective analysis of patients with acute brain injury and acute respiratory failure. Neurocrit Care. 2014; 21:186–191.
Article14. Grote E, Hassler W. The critical first minutes after subarachnoid hemorrhage. Neurosurgery. 1988; 22:654–661.
Article15. Nornes H. The role of intracranial pressure in the arrest of hemorrhage in patients with ruptured intracranial aneurysm. J Neurosurg. 1973; 39:226–234.
Article16. Csókay A, Nagy L, Vimláti L Jr. [Vascular tunnel creation to improve the effect of decompressive craniectomy in severe traumatic cerebral edema]. Orv Hetil. 2001; 142:75–78.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Meningioma With Partial and Spontaneous Regression of Peritumoral Edema on Long-Term Follow Up
- Radiological Characteristics of Peritumoral Edema in Meningiomas
- A Study of the Effects of Clinicobiological Factors upon the Meningioma-Associated Peritumoral Edema Formation
- Factors Influencing the Development of Peritumoral Brain Edema in Menigiomas
- A Meningioma With Extensive Peritumoral Edema Mimicking Metastatic Brain Tumor: A Case Report
