Spinal Extradural Arachnoid Cyst
- Affiliations
-
- 1Department of Neurosurgery, Pusan National University Yangsan Hospital, Yangsan, Korea. md6576@naver.com
- KMID: 2356799
- DOI: http://doi.org/10.13004/kjnt.2016.12.2.185
Abstract
- A spinal extradural arachnoid cyst (SEAC) results from a rare small defect of the dura matter that leads to cerebrospinal fluid accumulation and communication defects between the cyst and the subarachnoid space. There is consensus for the treatment of the dural defect, but not for the treatment of the cyst. Some advocate a total resection of the cysts and repair of the communication site to prevent the recurrence of a SEAC, while others recommended more conservative therapy. Here we report the outcomes of selective laminectomy and closure of the dural defect for a 72-year-old and a 33-year-old woman. Magnetic resonance imaging of these patients showed an extradural cyst from T12 to L4 and an arachnoid cyst at the posterior epidural space of T12 to L2. For both patients, we surgically fenestrated the cyst and repaired the dural defect using a partial hemi-laminectomy. The patient's symptoms dramatically subsided, and follow-up radiological images show a complete disappearance of the cyst in both patients. Our results suggest that fenestration of the cyst can be a safe and effective approach in treating SEACs compared to a classical complete resection of the cyst wall with multilevel laminectomy.
MeSH Terms
Figure
-
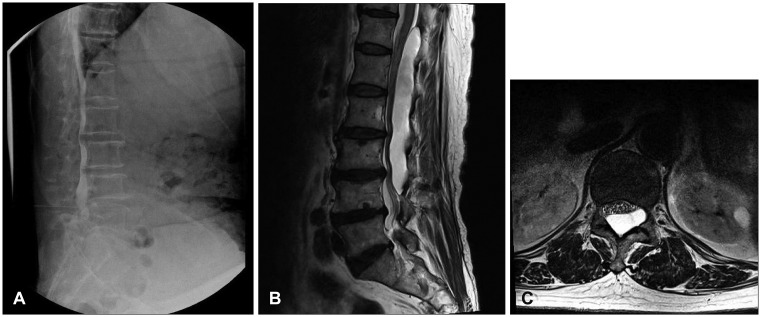
FIGURE 1 Preoperative images case 1. (A) Multi-level distortion of spinal canal and filling defect from T12 to L5 on myelogram. (B, C) Elongated cystic lesion compressing spinal thecal sac at T12 to L4.
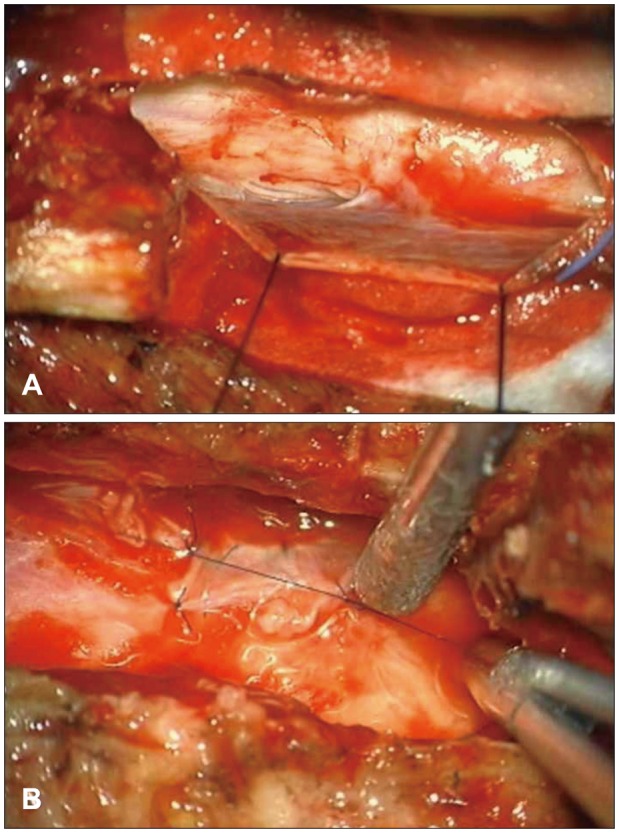
FIGURE 2 Intraoperative images of case 1. (A) L1 total laminectomy was performed to exposure dura defect. (B) Repair the defect site with the cyst wall.
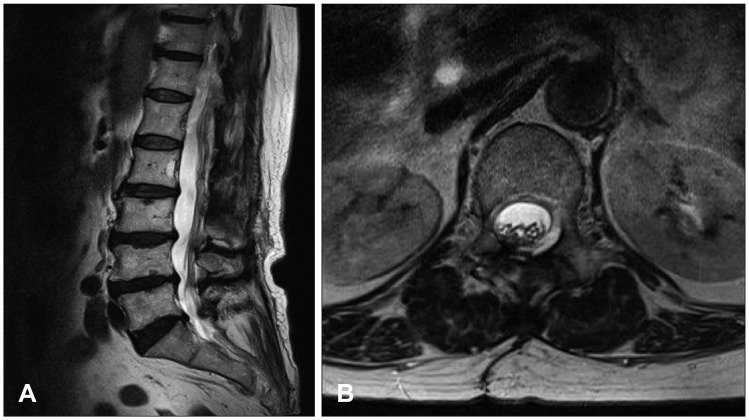
FIGURE 3 Postoperative images of case 1. (A, B) Magnetic resonance imaging taken 4 months after the surgery showed total removed state of cystic lesion.
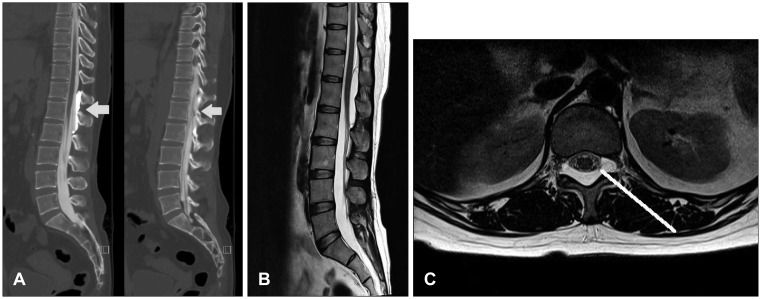
FIGURE 4 Preoperative images case 2. (A) Computed tomography myelography showed focal enhanced cystic mass that communicated with thecal sac at L1 level. (B, C) Cystic mass compressing dorsal side of thecal sac from T2 to L2 level.
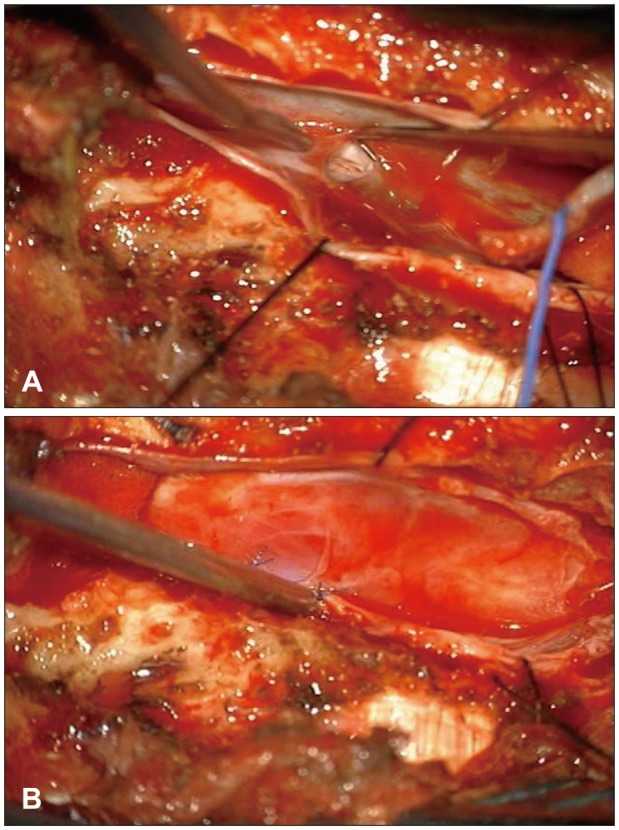
FIGURE 5 Intraoperative images of case 2. (A) Total laminectomy T12 and L1 level was performed to exposure the defective site. (B) Using cyst wall fragment, primary repair of defective site was performed.
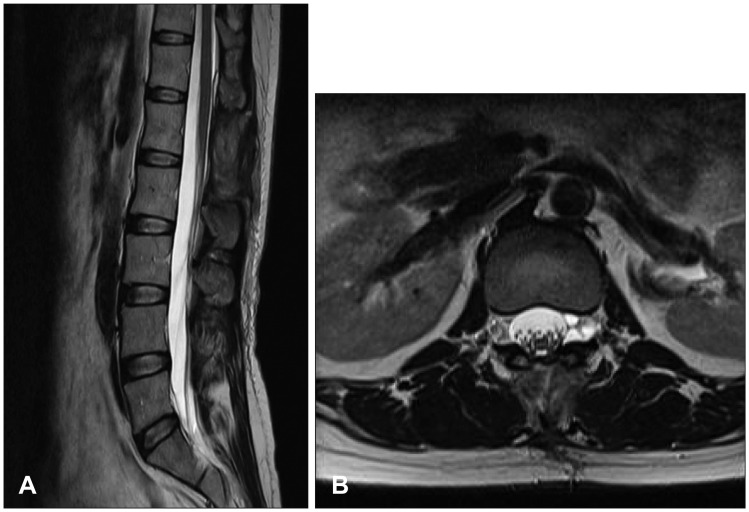
FIGURE 6 Postoperative images of case 2. (A, B) Magnetic resonance imaging taken 2 months after the surgery showed a complete disappearance of the cyst with no evidence of cord compression due to a residual cyst.
Cited by 2 articles
-
A Rare Cause of Thoracic Spinal Cord Compression by Multiple Large Tarlov Cysts
Ahmed-Salem Kleib, Sidi-Mohamed Salihy, Hussein Hamdi, Romain Carron, Outouma Soumaré
Korean J Neurotrauma. 2018;14(1):35-38. doi: 10.13004/kjnt.2018.14.1.35.Surgical Treatment of Ten Adults with Spinal Extradural Meningeal Cysts in the Thoracolumbar Spine
Feifan Xu, Fengzeng Jian, Liang Li, Jian Guan, Zan Chen
J Korean Neurosurg Soc. 2021;64(2):238-246. doi: 10.3340/jkns.2020.0244.
Reference
-
1. Choi SW, Seong HY, Roh SW. Spinal extradural arachnoid cyst. J Korean Neurosurg Soc. 2013; 54:355–358. PMID: 24294463.
Article2. Funao H, Nakamura M, Hosogane N, Watanabe K, Tsuji T, Ishii K, et al. Surgical treatment of spinal extradural arachnoid cysts in the thoracolumbar spine. Neurosurgery. 2012; 71:278–284. PMID: 22517249.
Article3. Furtado SV, Thakar S, Murthy GK, Dadlani R, Hegde AS. Management of complex giant spinal arachnoid cysts presenting with myelopathy. J Neurosurg Spine. 2011; 15:107–112. PMID: 21456891.
Article4. Kanetaka M, Sugita S, Chikuda H, Takeshita K, Ono T, Oshima Y, et al. Use of Doppler ultrasonography to detect an elusive communication of a spinal extradural arachnoid cyst. J Clin Neurosci. 2011; 18:863–864. PMID: 21489797.
Article5. Lee CH, Hyun SJ, Kim KJ, Jahng TA, Kim HJ. What is a reasonable surgical procedure for spinal extradural arachnoid cysts: is cyst removal mandatory? Eight consecutive cases and a review of the literature. Acta Neurochir (Wien). 2012; 154:1219–1227. PMID: 22573100.
Article6. Netra R, Min L, Shao Hui M, Wang JC, Bin Y, Ming Z. Spinal extradural meningeal cysts: an MRI evaluation of a case series and literature review. J Spinal Disord Tech. 2011; 24:132–136. PMID: 21430498.7. Ogura Y, Yabuki S, Iida A, Kou I, Nakajima M, Kano H, et al. FOXC2 mutations in familial and sporadic spinal extradural arachnoid cyst. PLoS One. 2013; 8:e80548. PMID: 24278289.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Septated Extradural Arachnoid Cyst in Thoracolumbar Spine Causing Myelopathy
- Extradural Spinal Arachnoid Cyst as a Cause of Cauda Equina Syndrome in a Child
- Multiple Extradural Arachnoid Cyst : A Case Report
- Retroperitoneal Spinal Extradural Arachnoid Cyst Combined with Congenital Hemivertebrae
- Huge Thoracolumbar Extradural Arachnoid Cyst
