J Gynecol Oncol.
2015 Oct;26(4):277-283. 10.3802/jgo.2015.26.4.277.
Controversies in the management of endometrial cancer: a survey of the Korean Gynecologic Oncology Group
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Institute of Women's Life Medical Science, Yonsei University College of Medicine, Seoul, Korea.
- 2Department of Obstetrics and Gynecology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
- 3Department of Obstetrics and Gynecology, Seoul Metropolitan Government Seoul National University Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea. tslee70@gmail.com
- 4Center for Uterine Cancer, National Cancer Center, Goyang, Korea.
- 5Department of Obstetrics and Gynecology, CHA Gangnam Medical Center, CHA University, Seoul, Korea.
- 6Department of Obstetrics and Gynecology, Seoul National University College of Medicine, Seoul, Korea.
- 7Department of Obstetrics and Gynecology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2345918
- DOI: http://doi.org/10.3802/jgo.2015.26.4.277
Abstract
OBJECTIVE
To identify current practice patterns for unresolved issues in the surgical and adjuvant management of endometrial cancer in Korea.
METHODS
We designed and conducted a survey of all 218 active members of the Korean Gynecologic Oncology Group to try to identify how they would manage various case scenarios for endometrial cancer. Data were collected using an Internet survey database.
RESULTS
A total of 108 members (49.5%) responded to the survey. Laparoscopy (81.6%) was the most commonly used mode of surgery in early-stage endometrial cancer. Of all the respondents, 19.8% stated that lymphadenectomy could be omitted and 21.7% recommended selective lymphadenectomy based on sentinel biopsy or frozen results for patients with presumed stage IA/grade 1 disease. On the other hand, 71.9% of respondents recommended para-aortic lymphadenectomy for patients with presumed stage IB/grade 1 disease and 86.4% recommended this treatment for presumed stage IB/grade 3 disease. The majority of respondents performed adjuvant therapy for stage IB/grade 2 (91.7%), IB/grade 3 (99.0%), and stage II (89.6%). Whole pelvic radiotherapy and vaginal brachytherapy were the most frequently used options among these patients. All respondents administered adjuvant therapy when node metastasis was found, and concurrent chemoradiotherapy (53.2%) was the most preferred option for stage IIIC1 disease.
CONCLUSION
There is broad variation in both the surgical and adjuvant treatment of endometrial cancer among Korean gynecologic oncologists.
Keyword
MeSH Terms
-
Adult
Combined Modality Therapy
Endometrial Neoplasms/pathology/*therapy
Female
*Gynecology
Humans
Incidental Findings
Lymph Node Excision/methods
Lymphatic Metastasis
Magnetic Resonance Imaging/methods
Male
Middle Aged
Neoadjuvant Therapy
Personal Satisfaction
Practice Patterns, Physicians'
Republic of Korea
Robotic Surgical Procedures
Figure
-
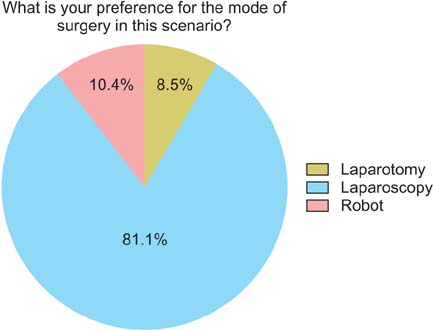
Fig. 1 Mode of surgery for presumed stage I disease.
Cited by 1 articles
-
Comparative Effectiveness of Abdominal versus Laparoscopic Radical Hysterectomy for Cervical Cancer in the Postdissemination Era
Jin Hee Kim, Kyungjoo Kim, Seo Jin Park, Jung-Yun Lee, Kidong Kim, Myong Cheol Lim, Jae Weon Kim
Cancer Res Treat. 2019;51(2):788-796. doi: 10.4143/crt.2018.120.
Reference
-
1. Lim MC, Moon EK, Shin A, Jung KW, Won YJ, Seo SS, et al. Incidence of cervical, endometrial, and ovarian cancer in Korea, 1999-2010. J Gynecol Oncol. 2013; 24:298–302.2. Lee JY, Kim EY, Jung KW, Shin A, Chan KK, Aoki D, et al. Trends in gynecologic cancer mortality in East Asian regions. J Gynecol Oncol. 2014; 25:174–182.3. Lee TS, Kim JW, Kim SH, Seong SJ, Song ES, Kim JH, et al. Surgical practice patterns in endometrial cancer: results of the Korean Gynecologic Oncology Group survey. J Gynecol Oncol. 2009; 20:107–112.4. Nout RA, Smit VT, Putter H, Jurgenliemk-Schulz IM, Jobsen JJ, Lutgens LC, et al. Vaginal brachytherapy versus pelvic external beam radiotherapy for patients with endometrial cancer of high-intermediate risk (PORTEC-2): an open-label, non-inferiority, randomised trial. Lancet. 2010; 375:816–823.5. ASTEC study group. Kitchener H, Swart AM, Qian Q, Amos C, Parmar MK. Efficacy of systematic pelvic lymphadenectomy in endometrial cancer (MRC ASTEC trial): a randomised study. Lancet. 2009; 373:125–136.6. Benedetti Panici P, Basile S, Maneschi F, Alberto Lissoni A, Signorelli M, Scambia G, et al. Systematic pelvic lymphadenectomy vs. no lymphadenectomy in early-stage endometrial carcinoma: randomized clinical trial. J Natl Cancer Inst. 2008; 100:1707–1716.7. Walker JL, Piedmonte MR, Spirtos NM, Eisenkop SM, Schlaerth JB, Mannel RS, et al. Recurrence and survival after random assignment to laparoscopy versus laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group LAP2 Study. J Clin Oncol. 2012; 30:695–700.8. Conrad LB, Ramirez PT, Burke W, Naumann RW, Ring KL, Munsell MF, et al. Role of minimally invasive surgery in gynecologic oncology: an updated survey of members of the Society of Gynecologic Oncology. Int J Gynecol Cancer. 2015; 25:1121–1127.9. Huh WK, Straughn JM Jr, Kelly FJ, Kilgore LC. Endometrial carcinoma. Curr Treat Options Oncol. 2001; 2:129–135.10. Sonoda Y. Surgical treatment for apparent early stage endometrial cancer. Obstet Gynecol Sci. 2014; 57:1–10.11. Fotopoulou C, Kraetschell R, Dowdy S, Fujiwara K, Yaegashi N, Larusso D, et al. Surgical and systemic management of endometrial cancer: an international survey. Arch Gynecol Obstet. 2015; 291:897–905.12. Soliman PT, Frumovitz M, Spannuth W, Greer MJ, Sharma S, Schmeler KM, et al. Lymphadenectomy during endometrial cancer staging: practice patterns among gynecologic oncologists. Gynecol Oncol. 2010; 119:291–294.13. Aalders J, Abeler V, Kolstad P, Onsrud M. Postoperative external irradiation and prognostic parameters in stage I endometrial carcinoma: clinical and histopathologic study of 540 patients. Obstet Gynecol. 1980; 56:419–427.14. Creutzberg CL, van Putten WL, Koper PC, Lybeert ML, Jobsen JJ, Warlam-Rodenhuis CC, et al. Surgery and postoperative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: multicentre randomised trial. PORTEC Study Group. Post Operative Radiation Therapy in Endometrial Carcinoma. Lancet. 2000; 355:1404–1411.15. ASTEC/EN.5 Study Group. Blake P, Swart AM, Orton J, Kitchener H, Whelan T, et al. Adjuvant external beam radiotherapy in the treatment of endometrial cancer (MRC ASTEC and NCIC CTG EN.5 randomised trials): pooled trial results, systematic review, and meta-analysis. Lancet. 2009; 373:137–146.16. Keys HM, Roberts JA, Brunetto VL, Zaino RJ, Spirtos NM, Bloss JD, et al. A phase III trial of surgery with or without adjunctive external pelvic radiation therapy in intermediate risk endometrial adenocarcinoma: a Gynecologic Oncology Group study. Gynecol Oncol. 2004; 92:744–751.17. Randall ME, Filiaci VL, Muss H, Spirtos NM, Mannel RS, Fowler J, et al. Randomized phase III trial of whole-abdominal irradiation versus doxorubicin and cisplatin chemotherapy in advanced endometrial carcinoma: a Gynecologic Oncology Group Study. J Clin Oncol. 2006; 24:36–44.18. Watanabe Y, Kitagawa R, Aoki D, Takeuchi S, Sagae S, Sakuragi N, et al. Practice pattern for postoperative management of endometrial cancer in Japan: a survey of the Japanese Gynecologic Oncology Group. Gynecol Oncol. 2009; 115:456–459.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A critical assessment on the role of sentinel node mapping in endometrial cancer
- Response to comment on: Comparison of diagnostic accuracy between endometrial curettage and aspiration biopsy in patients treated with progestin for endometrial hyperplasia: a Korean Gynecologic Oncology Group study
- Letter to editor in response to: Comparison of diagnostic accuracy between endometrial curettage and aspiration biopsy in patients treated with progestin for endometrial hyperplasia: a Korean Gynecologic Oncology Group study
- Present status and future direction of clinical trials in advanced endometrial carcinoma
- Gynecologic oncology group trials in uterine corpus malignancies: recent progress
