Tuberc Respir Dis.
2014 Jan;76(1):38-41.
A Case of Immunoglobulin G4-Related Disease Presenting as a Pleural Mass
- Affiliations
-
- 1Department of Internal Medicine, KEPCO Medical Center, Seoul, Korea. humanmd04@hanmail.net
- 2Department of Pathology, KEPCO Medical Center, Seoul, Korea.
- 3Division of Respiratory and Critical Care Medicine, Seoul National University Bundang Hospital, Seoul, Korea.
Abstract
- Immunoglobulin G4 (IgG4)-related disease is a newly recognized condition characterized by fibroinflammatory lesions with dense lymphoplasmacytic infiltration, storiform-type fibrosis and obliterative phlebitis. The pathogenesis is not fully understood but multiple immune-mediated mechanisms are believed to contribute. This rare disease can involve various organs and pleural involvement is even rarer. We report a case of IgG4-related disease involving pleura. A 66-year-old man presented with cough and sputum production for a week. Chest radiography revealed consolidation and a pleural mass at right hemithorax. Treatment with antibiotics resolved the consolidation and respiratory symptoms disappeared, but the pleural mass was unchanged. Video-assisted thoracoscopic surgery was performed. Histopathology revealed dense lymphoplasmacytic infiltration and storiform fibrosis with numerous IgG4-bearing plasma cells. The serum IgG4 level was also elevated. Further examination ruled out the involvement of any other organ. The patient was discharged without further treatment and there is no evidence of recurrence to date.
MeSH Terms
Figure
-

Figure 1 Chest radiography showed a well-defined nodular opacity in right upper hemithorax (arrow) and consolidation at right lower lobe (asterisk).
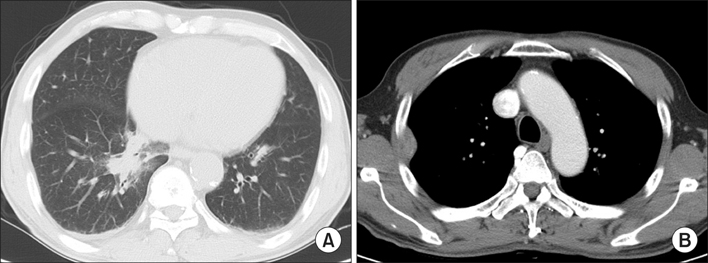
Figure 2 Chest computed tomography scan showed a consolidative lesion at right lower lobe (A) and a pleura-based mass with contrast enhancement surrounding normal lung parenchyma in right upper lobe (B).

Figure 3 Histopathologic examination showed dense infiltration of inflammatory cells consisting mainly of lymphocytes and plasma cells with some eosinophils (A), and characteristic storiform-type fibrosis (B) (A, B; H&E stain, ×200; inset in A, ×400). In immunohistochemical staining, numerous IgG- and IgG4-positive plasma cells were identified (C, D) (×200).
Reference
-
1. Hamano H, Kawa S, Horiuchi A, Unno H, Furuya N, Akamatsu T, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001; 344:732–738.2. Zen Y, Harada K, Sasaki M, Sato Y, Tsuneyama K, Haratake J, et al. IgG4-related sclerosing cholangitis with and without hepatic inflammatory pseudotumor, and sclerosing pancreatitis-associated sclerosing cholangitis: do they belong to a spectrum of sclerosing pancreatitis? Am J Surg Pathol. 2004; 28:1193–1203.3. Kitagawa S, Zen Y, Harada K, Sasaki M, Sato Y, Minato H, et al. Abundant IgG4-positive plasma cell infiltration characterizes chronic sclerosing sialadenitis (Kuttner's tumor). Am J Surg Pathol. 2005; 29:783–791.4. Kasashima S, Zen Y, Kawashima A, Konishi K, Sasaki H, Endo M, et al. Inflammatory abdominal aortic aneurysm: close relationship to IgG4-related periaortitis. Am J Surg Pathol. 2008; 32:197–204.5. Kamisawa T, Funata N, Hayashi Y, Eishi Y, Koike M, Tsuruta K, et al. A new clinicopathological entity of IgG4-related autoimmune disease. J Gastroenterol. 2003; 38:982–984.6. Deshpande V, Zen Y, Chan JK, Yi EE, Sato Y, Yoshino T, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012; 25:1181–1192.7. Sah RP, Chari ST. Serologic issues in IgG4-related systemic disease and autoimmune pancreatitis. Curr Opin Rheumatol. 2011; 23:108–113.8. Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med. 2012; 366:539–551.9. Zen Y, Inoue D, Kitao A, Onodera M, Abo H, Miyayama S, et al. IgG4-related lung and pleural disease: a clinicopathologic study of 21 cases. Am J Surg Pathol. 2009; 33:1886–1893.10. Kobayashi H, Shimokawaji T, Kanoh S, Motoyoshi K, Aida S. IgG4-positive pulmonary disease. J Thorac Imaging. 2007; 22:360–362.11. Inoue D, Zen Y, Abo H, Gabata T, Demachi H, Kobayashi T, et al. Immunoglobulin G4-related lung disease: CT findings with pathologic correlations. Radiology. 2009; 251:260–270.12. Fukui T, Mitsuyama T, Takaoka M, Uchida K, Matsushita M, Okazaki K. Pancreatic cancer associated with autoimmune pancreatitis in remission. Intern Med. 2008; 47:151–155.13. Cheuk W, Yuen HK, Chan AC, Shih LY, Kuo TT, Ma MW, et al. Ocular adnexal lymphoma associated with IgG4+ chronic sclerosing dacryoadenitis: a previously undescribed complication of IgG4-related sclerosing disease. Am J Surg Pathol. 2008; 32:1159–1167.14. Kamisawa T, Anjiki H, Egawa N, Kubota N. Allergic manifestations in autoimmune pancreatitis. Eur J Gastroenterol Hepatol. 2009; 21:1136–1139.15. Kamisawa T, Shimosegawa T, Okazaki K, Nishino T, Watanabe H, Kanno A, et al. Standard steroid treatment for autoimmune pancreatitis. Gut. 2009; 58:1504–1507.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Recurrent Ischemic Stroke Associated with Immunoglobulin G4-Related Disease
- Immunoglobulin G4-Related Inflammatory Pseudotumor Presenting as a Solitary Mass in the Stomach
- Immunoglobulin G4-Related Kidney Disease with Membranous Proliferative Glomerulonephritis Presenting with a Renal Pelvic Mass
- Unusual Manifestation of Immunoglobulin G4-Related Disease Involving the Retroperitoneum: A Case Report
- Unusual Manifestation of Immunoglobulin G4-Related Disease Involving the Upper Arm: A Case Report
