A Case of Atypical Adenomatous Hyperplasia of Larger Than 2 cm
- Affiliations
-
- 1Department of Internal Medicine, Chungnam National University School of Medicine, Daejeon, Korea. jss24@cnuh.co.kr
- 2Department of Pathology, Chungnam National University School of Medicine, Daejeon, Korea.
Abstract
- Atypical adenomatous hyperplasia (AAH) has been considered to be a precursor lesion of bronchioloalveolar carcinoma (BAC) and pulmonary adenocarcinoma. It usually coexists with BAC and/or an adenocarcinoma. Chest computed tomography reveals multiple well-defined nodules with ground-glass opacity. Usually, AAH does not exceed 10 mm in size. AAH with extensive involvement on one side of the lung field or one that is larger than 2 cm has not been previously reported. We herein report a case of a 71-year-old nonsmoking female with lung AAH of larger than 2 cm.
Keyword
MeSH Terms
Figure
-
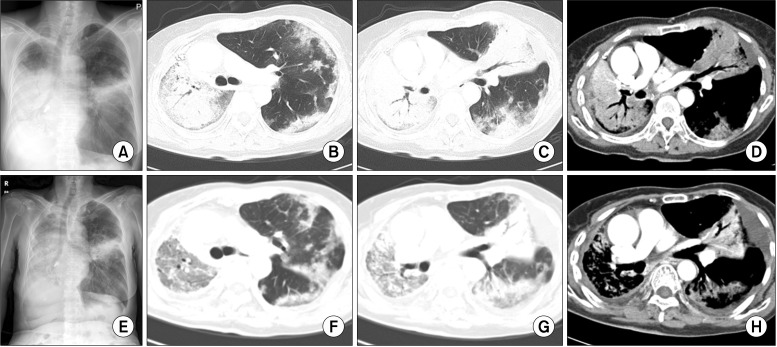
Figure 1 Chest posteroanterior (PA) view and chest computed tomography (CT). (A) Chest PA on first admission. Patient revisited for aggravation of dyspnea on exertion. Widening of haziness in the right lower lung field and aggravation of linear infiltration in the left middle lung field were shown. (B-D) Chest CT on first admission. Airspace consolidation in the right lung and lingular division of the left upper lobe were shown on the CT. Collapse of the right middle lobe and right lower lobe was noted. Multiple variably sized nodules, some well-defined and some ill-defined, with patchy consolidation and ground-glass opacity (GGO) are present in both the upper lobe and left lower lobe (LLL). (E) Chest PA on second admission. (F-H) Improvement of consolidation in the right lung field, but increased extent of GGO in the right upper lobe and LLL were noted on chest CT at the second admission.
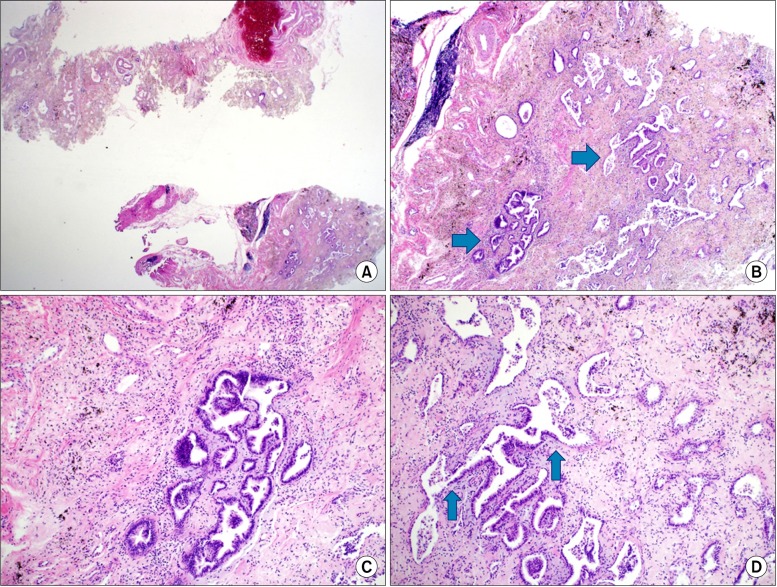
Figure 2 Pathologic findings of the surgical lung biopsy specimen and microscopic findings upon hematoxylin and eosin staining. (A) Overall fibrosis and focal atypical alveolar epithelium are noted. (B) Atypical alveolar epithelium (arrows). (C) Magnified atypical alveolar epithelium. (D) Transition area from normal to atypical alveolar epithelium (arrows).
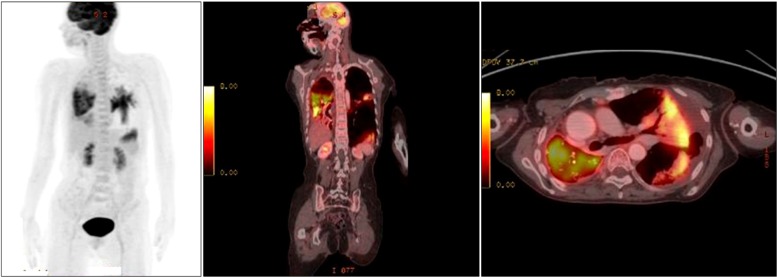
Figure 3 Increased glucose metabolism in the right middle and lower lung zones and lateral and posterobasal segment of the left lower lobe are shown using positron emission tomography-computed tomography.

Figure 4 Chest radiograph in 17 days after gefitinib treatment.
Reference
-
1. Brambilla E, Travis WD, Colby TV, Corrin B, Shimosato Y. The new World Health Organization classification of lung tumours. Eur Respir J. 2001; 18:1059–1068. PMID: 11829087.
Article2. Chapman AD, Kerr KM. The association between atypical adenomatous hyperplasia and primary lung cancer. Br J Cancer. 2000; 83:632–636. PMID: 10944604.
Article3. Kawakami S, Sone S, Takashima S, Li F, Yang ZG, Maruyama Y, et al. Atypical adenomatous hyperplasia of the lung: correlation between high-resolution CT findings and histopathologic features. Eur Radiol. 2001; 11:811–814. PMID: 11372613.
Article4. Ishikawa H. Pathologic/high-resolution CT correlation of focal lung lesions 5 mm or less in diameter: detection and identification by multidetector-row CT. Nihon Igaku Hoshasen Gakkai Zasshi. 2002; 62:415–422. PMID: 12187837.5. Jung KW, Park S, Kong HJ, Won YJ, Lee JY, Park EC, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2008. Cancer Res Treat. 2011; 43:1–11. PMID: 21509157.
Article6. Ishikawa H, Koizumi N, Naito M, Umezu H, Morita T, Nemoto T, et al. High-resolution CT findings of pulmonary atypical adenomatous hyperplasia of 5 mm or less in diameter. Nihon Igaku Hoshasen Gakkai Zasshi. 2003; 63:311–315. PMID: 12934549.7. Park CM, Goo JM, Lee HJ, Lee CH, Kim HC, Chung DH, et al. CT findings of atypical adenomatous hyperplasia in the lung. Korean J Radiol. 2006; 7:80–86. PMID: 16799268.
Article8. Kayser K, Nwoye JO, Kosjerina Z, Goldmann T, Vollmer E, Kaltner H, et al. Atypical adenomatous hyperplasia of lung: its incidence and analysis of clinical, glycohistochemical and structural features including newly defined growth regulators and vascularization. Lung Cancer. 2003; 42:171–182. PMID: 14568684.
Article9. Bae SH, Jung KJ, Bae JY. Multiple atypical adenomatous hyperplasia mimicking lung to lung metastasis: a case report. Korean J Pathol. 2005; 39:203–206.10. Han AR, Kwon OJ, Kwon YS, Shin J, Koh WJ, Cho EY, et al. An atypical adenomatous hyperplasia presenting as a solitary pulmonary nodule with ground glass opacity. Korean J Med. 2007; 72(Suppl 2):S221–S224.11. Lee HS, Choi JS, Seo KH, Na JO, Kim YH, Oh MH, et al. A case of congenital cystic adenomatoid malformation of the lng with atypical adenomatous hyperplasia in adult. Tuberc Respir Dis. 2009; 66:385–389.
Article12. Nomori H, Horio H, Naruke T, Suemasu K, Morinaga S, Noguchi M. A case of multiple atypical adenomatous hyperplasia of the lung detected by computed tomography. Jpn J Clin Oncol. 2001; 31:514–516. PMID: 11696623.
Article13. Seki M, Akasaka Y. Multiple lung adenocarcinomas and AAH treated by surgical resection. Lung Cancer. 2007; 55:237–240. PMID: 17118487.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Solitary Atypical Adenomatous Hyperplasia in a 12-Year-Old Girl
- Cytological features of atypical adenomatous hyperplasia and adenocarcinoma in situ of the lung: a case report
- Multiple Atypical Adenomatous Hyperplasia Mimicking Lung to Lung Metastasis: A Case Report
- A Case of Atypical Melanocytic Hyperplasia
- Adenomatous Hyperplasia Arising from Dual Ectopic Thyroid
