Tuberc Respir Dis.
2008 Oct;65(4):308-312.
A Case of Bilateral Gynecomastia Associated with Isoniazid
- Affiliations
-
- 1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
- 2Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul Metropolitan Government Seoul National University Boramae Medical Center, Seoul, Korea. kimdkmd@snu.ac.kr
Abstract
- Gynecomastia is a benign enlargement of the male breast attributable to proliferation of the ductal elements. Gynecomastia has been rarely reported as an adverse effect of isoniazid therapy. We report the case of a 35-year-old man who was prescribed with isoniazid, rifampicin, ethambutol and pyrazinamide to treat pulmonary and lymphatic tuberculosis. After five months of treatment, the patient complained of painful engorgement in the bilateral breasts and the presence of male gynecomastia was confirmed with a physical examination and radiographical methods. The serum level of estradiol was also increased. Common causes of male gynecomastia were excluded through history taking and the laboratory findings. The anti-TB drugs were changed to a second line regimen due to radiographical progression and the intolerance of the patient to gynecomastia. Gynecomastia was relieved very slowly and a tender subareolar palpable mass decreased in size and consistency over five-month period after stopping the probable causative drug, isoniazid. From a review of the literature, gynecomastia has been shown to be a side effect of treatment with first line anti-tuberculosis drugs, and especially with isoniazid. We report the rare case.
Keyword
MeSH Terms
Figure
-
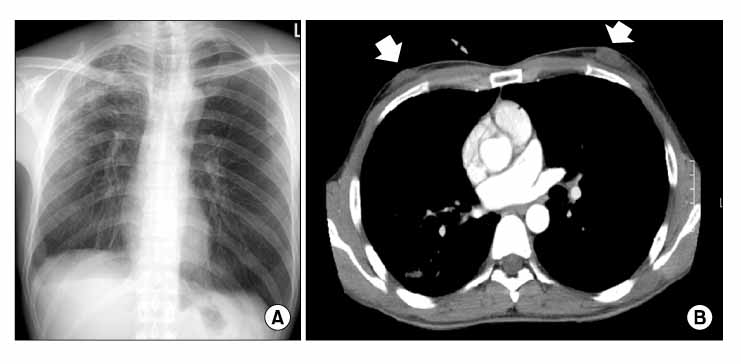
Figure 1 Chest PA and enhanced Chest CT scan. (A) Multiple ill defined patchy and nodular densities in the BULF. (B) Enlarged soft tissue mass shadow in both breasts were visualized on enhanced chest CT (arrows).
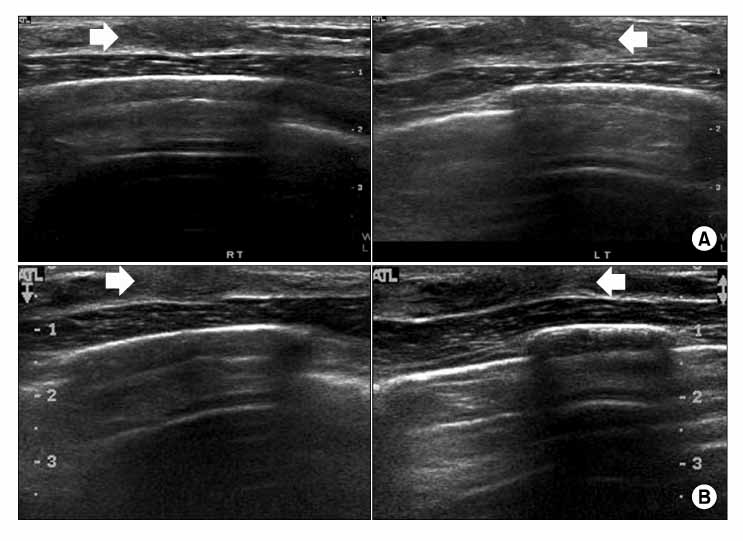
Figure 2 Breast ultrasonography. (A) Initial: The enlarged breasts were attributable to proliferation of the hyperechoic ductular elements (arrows) and not merely excessive breast adipose tissue. (B) Follow up: Both minimal gynecomastia, but decreased proliferation of the ductular elements (arrows), 8 months after discontinued Isoniazid.
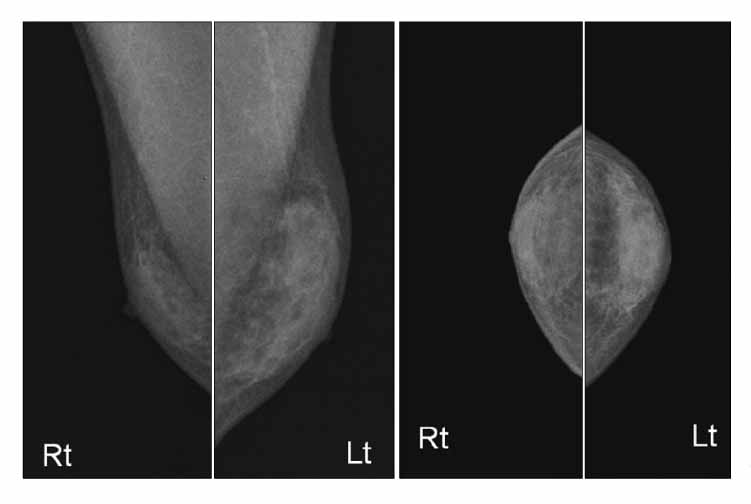
Figure 3 Mammography. Mammography showed the proliferated subareolar ductal structure.
Reference
-
1. American Thoracic Society, CDC, Infectious Diseases Society of America. Treatment of tuberculosis. MMWR Recomm Rep. 2003. 52:1–77.2. Khanna P, Panjabi C, Maurya V, Shah A. Isoniazid asso ciated, painful, bilateral gynaecomastia. Indian J Chest Dis Allied Sci. 2003. 45:277–279.3. Garg R, Mehra S, Prasad R. Isoniazid induced gynaecomastia: a case report. Internet J Pharmacol. 2008. 5(2):4. Bergogne-Berezin E, Nouhouayi A, Letonturier P, Thibault B, Tourneur R. Gynecomastia caused by isoniazid. Value of determination of the inactivation phenotype. Nouv Presse Med. 1976. 5:213–214.5. Guinet P, Garin JP, Morneix A. Gynecomastia in a grave case of pulmonary tuberculosis during isonicotinic hydrazide therapy. Lyon Med. 1953. 188:281–284.6. Braunstein GD. Gynecomastia. N Engl J Med. 1993. 328:490–495.7. Braunstein GD. Clinical practice. Gynecomastia. N Engl J Med. 2007. 357:1229–1237.8. Narula HS, Carlson HE. Gynecomastia. Endocrinol Metab Clin North Am. 2007. 36:497–519.9. Bembo SA, Carlson HE. Gynecomastia: its features, and when and how to treat it. Cleve Clin J Med. 2004. 71:511–517.10. Braunstein GD. Aromatase and gynecomastia. Endocr Relat Cancer. 1999. 6:315–324.11. Nicolis GL, Modlinger RS, Gabrilove JL. A study of the histopathology of human gynecomastia. J Clin Endocrinol Metab. 1971. 32:173–178.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Isoniazid Induced Gynecomastia
- Two Cases of ReVersible Bilateral Painful Gynecomastia Induced by 1mg Oral Finasteride(Propecia(R))
- Gynecomastia: A Rare Adverse Effect of Methylphenidate in an Adolescent Boy
- Hyperkeratosis of Nipple and Areola in a Man with Gynecomastia
- Idiopathic Unilateral Gynecomastia in an Adolescent Male: A Case Report
