J Dent Anesth Pain Med.
2016 Mar;16(1):1-8. 10.17245/jdapm.2016.16.1.1.
Diagnosis and treatment of abnormal dental pain
- Affiliations
-
- 1Division of Special Needs Dentistry and Orofacial Pain, Department of Oral Health and Clinical Science, Tokyo Dental College, Tokyo, Japan. kfukuda@tdc.ac.jp
- KMID: 2308759
- DOI: http://doi.org/10.17245/jdapm.2016.16.1.1
Abstract
- Most dental pain is caused by an organic problem such as dental caries, periodontitis, pulpitis, or trauma. Diagnosis and treatment of these symptoms are relatively straightforward. However, patients often also complain of abnormal dental pain that has a non-dental origin, whose diagnosis is challenging. Such abnormal dental pain can be categorized on the basis of its cause as referred pain, neuromodulatory pain, and neuropathic pain. When it is difficult to diagnose a patient's dental pain, these potential alternate causes should be considered. In this clinical review, we have presented a case of referred pain from the digastric muscle (Patient 1), of pulpectomized (Patient 2), and of pulpectomized pain (Patient 3) to illustrate referred, neuromodulatory, and neuropathic pain, respectively. The Patient 1 was advised muscle stretching and gentle massage of the trigger points, as well as pain relief using a nonsteroidal anti-inflammatory and the tricyclic antidepressant amitriptyline. The pain in Patient 2 was relieved completely by the tricyclic antidepressant amitriptyline. In Patient 3, the pain was controlled using either a continuous drip infusion of adenosine triphosphate or intravenous Mg2+ and lidocaine administered every 2 weeks. In each case of abnormal dental pain, the patient's diagnostic chart was used (Fig.2 and 3). Pain was satisfactorily relieved in all cases.
Keyword
MeSH Terms
Figure
-
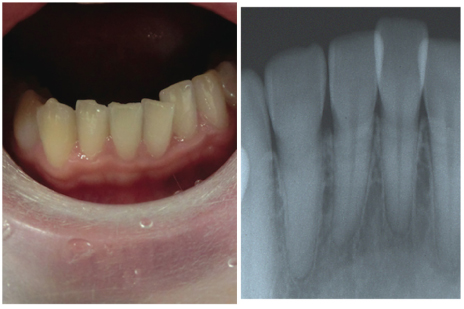
Fig. 1 A 28 year-old female with the complaint, "My lower central incisors hurt".
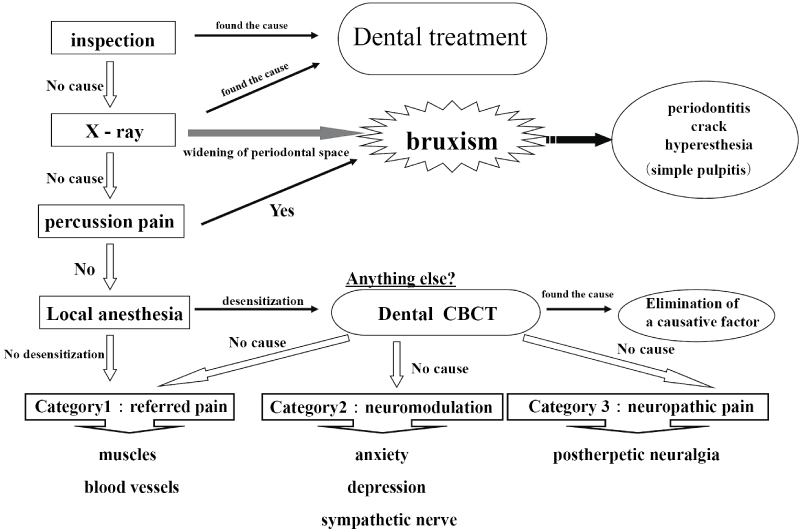
Fig. 2 Diagnostic chart for abnormal dental pain.
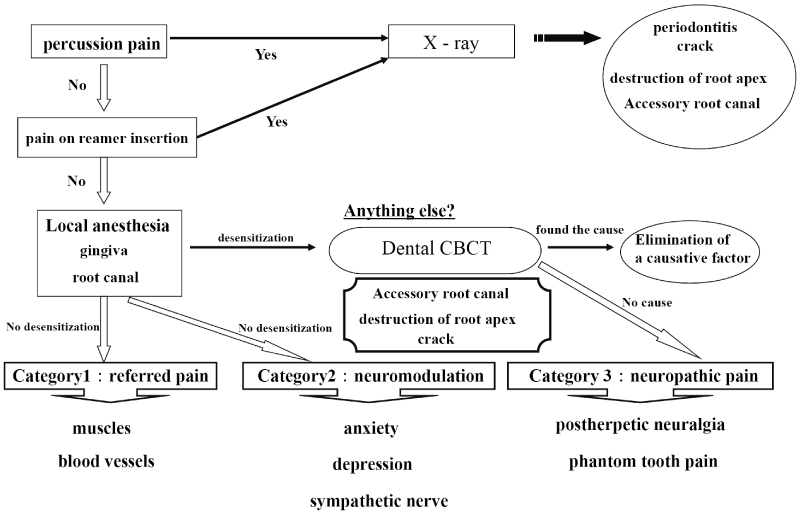
Fig. 3 Diagnostic chart for abnormal pulpectomized dental pain.
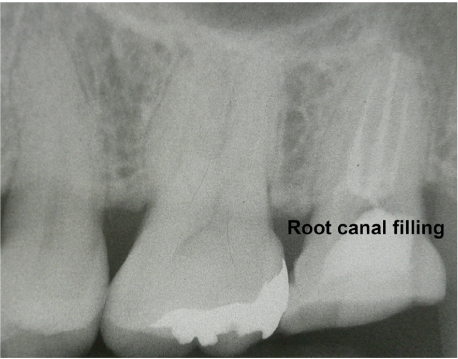
Fig. 4 The root canal was filled without incident.
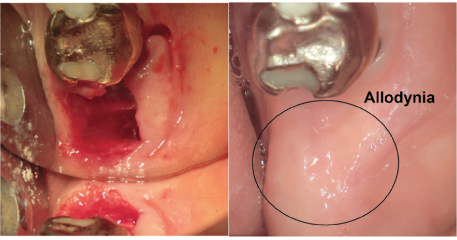
Fig. 5 Allodynia was obsereved on mucosal surfaces following the extraction.
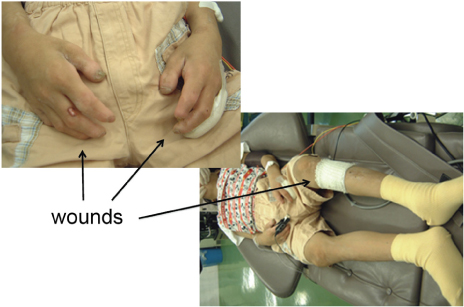
Fig. 6 A patient with congenital insensitivity to pain with anhidrosis.
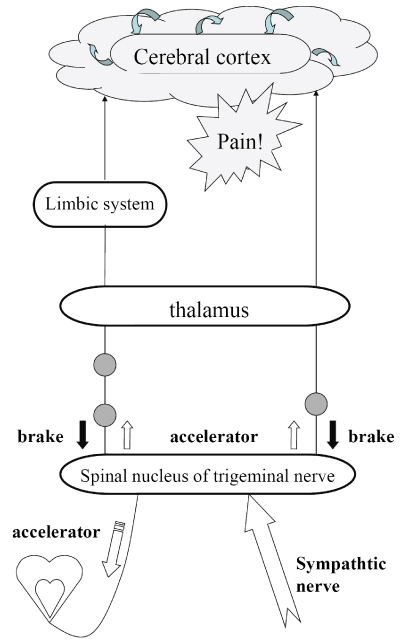
Fig. 7 Mechanism that produces pain.
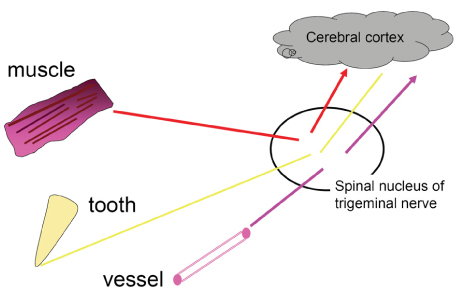
Fig. 8 Information transmitted from various sites is bundled together at the synapses of trigeminal nerve.
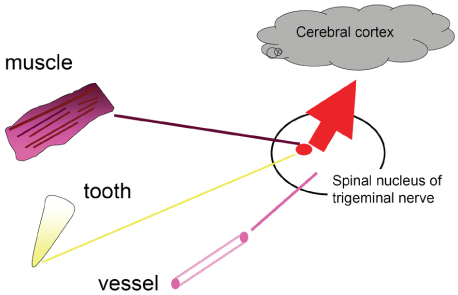
Fig. 9 Referred Pain.
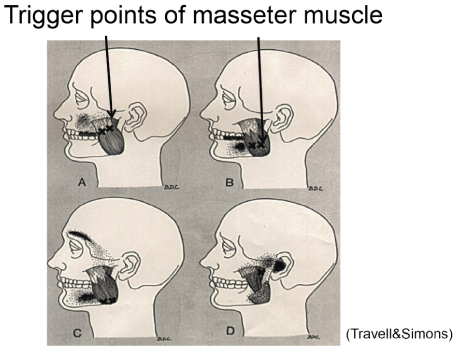
Fig. 10 Trigger point of masseter muscle.
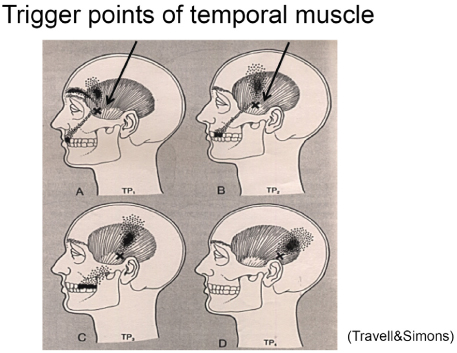
Fig. 11 Trigger point of temporal muscle.
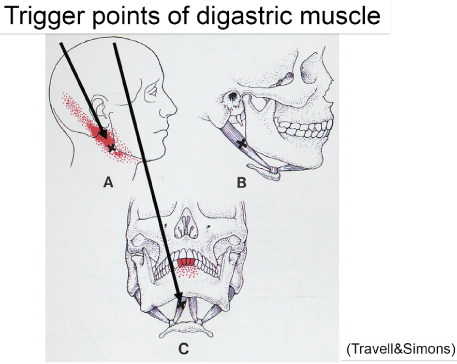
Fig. 12 Trigger point of digastric muscle.
Reference
-
1. Fukuda K, Hayashida M, Fukunaga A, Kasahara M, Ichinohe T, Kaneko Y. Pain-relieving effects of intravenous adenosine 5'-triphosphate (ATP) in chronic intractable orofacial pain: an open-label study. J Anesth. 2007; 21:24–30.2. Travell JG, Simons DG. Myofascial Pain and Disfunction: The Trigger Point Manual. 1st ed. Baltimore: Williams and Wilkins;1983.3. Fukuda K, Ichinohe T, Kaneko Y. Pain management for nerve injury following dental implant surgery at Tokyo Dental College Dental College Hospital. Int J Dent. 2012; 2012:209474.
Article4. Marbach JJ, Hulbrock J, Hohn C, Segal AG. Incidence of phantom tooth pain: an atypical facial neuralgia. Oral Surg Oral Med Oral Pathol. 1982; 53:190–193.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- An Insight Into Neurophysiology of Pulpal Pain: Facts and Hypotheses
- Analysis of Final Diagnosis of Patients with Suspected Nonodontogenic Toothache: A Retrospective Study
- Assessment of Risk Factors for Dental Developmental Disorders in Pediatric Cancer Survivors
- Clinical Features of the Persistent Idiopathic Dentoalveolar Pain Compared with Inflammatory Dental Pain
- Treatment of severe pain in a patient with complex regional pain syndrome undergoing dental treatment under general anesthesia: A case report
