Determination of Safe Contrast Media Dosage to Estimated Glomerular Filtration Rate Ratios to Avoid Contrast-Induced Nephropathy After Elective Percutaneous Coronary Intervention
- Affiliations
-
- 1Devision of Cardiology, Department of Internal Medicine, Keimyung University Dongsan Medical Center, Daegu, Korea. shur@dsmc.or.kr
- KMID: 2297934
- DOI: http://doi.org/10.4070/kcj.2011.41.5.265
Abstract
- BACKGROUND AND OBJECTIVES
To avoid the risk of developing contrast-induced nephropathy (CIN), it has been suggested that patients be subjected to a minimal necessary dose of contrast medium (CM-dose). However, often it is not easy to determine such a dose. This study assessed the usefulness of the ratio of CM-dose to estimated glomerular filtration rate (eGFR) in predicting the risks of CIN and sought to determine the safe level of CM-dose/eGFR in patients undergoing non-emergent percutaneous coronary intervention (PCI).
SUBJECTS AND METHODS
We enrolled a total of 226 patients and calculated the ratio of CM-dose using grams of iodine (g-I) to eGFR, thus expressing it as g-I/eGFR. Among the CIN patients, those with ne-phropathy requiring dialysis (NRD) were also evaluated.
RESULTS
Overall, there were 16 cases (7.1%) of CIN. On univariate and multivariate regression analysis, g-I/eGFR alone was found to be an independent predictor for CIN (hazard ratio=10.73, p<0.001). In an receiver operating characteristic analysis, fair discrimination for CIN was found at a g-I/eGFR level of 1.42 (C statics=0.867), and at this value, the sensitivity and specificity were 81.3% and 80%, respectively. Of patients (n=51) with g-I/eGFR > or =1.42, 23.6% (13/51) and 7.8% (4/51) developed, while those with g-I/eGFR <1.42 (n=171) had a lower incidences of CIN (1.8%, 2/171, p<0.001) and NRD (0%, 0/171, p<0.001).
CONCLUSION
It can be concluded that a g-I/eGFR <1.42 is a simple, useful indicator for determining the safe CM-dose based on the pre-PCI eGFR values. Furthermore, g-I/eGFR might have a close relationship with the development of NRD as well as CIN.
MeSH Terms
Figure
-

Fig. 1 Incidence of CIN according to quartiles of g-I/eGFR. Incidence of CIN is markedly higher in quartiles III and IV compared with quartiles I and II. CIN: contrast-induced nephropathy, g-I/eGFR: ratio of delivered contrast media by grams of iodine and estimated glomerular filtration rate.
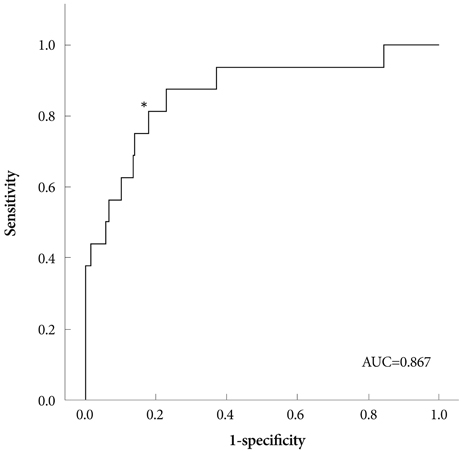
Fig. 2 Receiver operating characteristic curves for the prediction of CIN using a g-I/eGFR ratio. The area under the curve for predicting CIN of g-I/eGFR was 0.867. The best cut-off value for g-I/eGFR was determined to be 1.42 (*). At this value, the sensitivity and specificity for the development of CIN were 81.3% and 80%, respectively. AUC: area under the curve, CIN: contrast-induced nephropathy, g-I/eGFR: ratio of delivered contrast media by grams of iodine and estimated glomerular filtration rate.
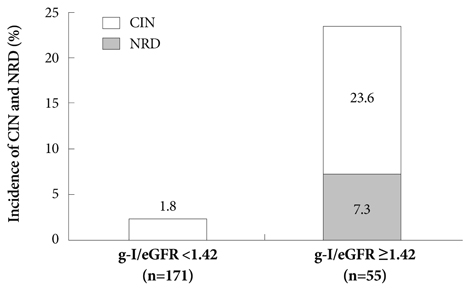
Fig. 3 Depiction of the incidence for CIN and NRD according to g-I/eGFR. Of patients with g-I/eGFR ≥1.42, there were significantly higher incidences of CIN and NRD compared with patients with g-I/eGFR <1.42 (p<0.001). CIN: contrast-induced nephropathy, NRD: nephropathy requiring dialysis, g-I/eGFR: ratio of delivered contrast media by grams of iodine and estimated glomerular filtration rate.

Fig. 4 Relationship between the g-I/eGFR ratio and clinical course after exposure to contrast Medium. g-I/eGFR levels (mean±SD) were significantly correlated with clinical courses of renal complication after PCI. g-I/eGFR: ratio of delivered contrast media by grams of iodine and estimated glomerular filtration rate, CIN: contrast-induced nephropathy, PCI: percutaneous coronary intervention.
Reference
-
1. Murphy SW, Barrett BJ, Parfrey PS. Contrast nephropathy. J Am Soc Nephrol. 2000. 11:177–182.2. Porter GA. Contrast-associated nephropathy: presentation, pathophysiology and management. Miner Electrolyte Metab. 1994. 20:232–243.3. McCullough PA, Wolyn R, Rocher LL, Levin RN, O'Neill WW. Acute renal failure after coronary intervention: incidence, risk factors, and relationship to mortality. Am J Med. 1997. 103:368–375.4. McCullough PA, Adam A, Becker CR, et al. Epidemiology and prognostic implications of contrast-induced nephropathy. Am J Cardiol. 2006. 98:5K–13K.5. Rihal CS, Textor SC, Grill DE, et al. Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation. 2002. 105:2259–2264.6. Dangas G, Iakovou I, Nikolsky E, et al. Contrast-induced nephropathy after percutaneous coronary interventions in relation to chronic kidney disease and hemodynamic variables. Am J Cardiol. 2005. 95:13–19.7. Morcos SK. Contrast media-induced nephrotoxicity: questions and answers. Br J Radiol. 1998. 71:357–365.8. Lee KH, Lee SR, Kang KP, et al. Periprocedural hemoglobin drop and contrast-induced nephropathy in percutaneous coronary intervention patients. Korean Circ J. 2010. 40:68–73.9. Namgung J, Doh JH, Lee SY, Hur WS, Park SW, Lee WR. Effect of N-acetylcysteine in prevention of contrast-induced nephropathy after coronary angiography. Korean Circ J. 2005. 35:696–701.10. Kelly AM, Dwamena B, Cronin P, Bernstein SJ, Carlos RC. Meta-analysis: effectiveness of drugs for preventing contrast-induced nephropathy. Ann Intern Med. 2008. 148:284–294.11. Cigarroa RG, Lange RA, Williams RH, Hillis LD. Dosing of contrast material to prevent contrast nephropathy in patients with renal disease. Am J Med. 1989. 86:649–652.12. Altmann D, Zwas D, Spatz A, et al. Use of the contrast volume estimated creatinine clearance ratio to predict renal failure after angiography. J Interv Cardiol. 1997. 10:113–119.13. Bartholomew BA, Harjai KJ, Dukkipati S, et al. Impact of nephropathy after percutaneous coronary intervention and a method for risk stratification. Am J Cardiol. 2004. 93:1515–1519.14. Laskey WK, Jenkins C, Selzer F, et al. Volume-to-creatinine clearance ratio: a pharmacokinetically based risk factor for prediction of early creatinine increase after percutaneous coronary intervention. J Am Coll Cardiol. 2007. 50:584–590.15. Nyman U, Almen T, Aspelin P, Hellstrom M, Kristiansson M, Sterner G. Contrast-medium-Induced nephropathy correlated to the ratio between dose in gram iodine and estimated GFR in ml/min. Acta Radiol. 2005. 46:830–842.16. Kim U, Kim YJ, Lee WJ, et al. The estimated glomerular filtration rate with using the Mayo clinic quardratic equation as a new predictor for developing contrast induced nephropathy in patients with angina pectoris. Korean Circ J. 2008. 38:301–304.17. McCullough PA. Contrast-induced acute kidney injury. J Am Coll Cardiol. 2008. 51:1419–1428.18. Levey AS, Greene T, Schluchter MD, et al. Glomerular filtration rate measurements in clinical trials. Modification of Diet in Renal Disease Study Group and the Diabetes Control and Complications Trial Research Group. J Am Soc Nephrol. 1993. 4:1159–1171.19. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. Modification of Diet in Renal Disease Study Group. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Intern Med. 1999. 130:461–470.20. Frennby B, Sterner G. Contrast media as markers of GFR. Eur Radiol. 2002. 12:475–484.21. Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976. 16:31–41.22. Nyman U, Bjork J, Aspelin P, Marenzi G. Contrast medium dose-to-GFR ratio: a measure of systemic exposure to predict contrast-induced nephropathy after percutaneous coronary intervention. Acta Radiol. 2008. 49:658–667.23. Barrett BJ, Carlisle EJ. Metaanalysis of the relative nephrotoxicity of high- and low-osmolality iodinated contrast media. Radiology. 1993. 188:171–178.24. Liss P, Persson PB, Hansell P, Lagerqvist B. Renal failure in 57,925 patients undergoing coronary procedures using iso-osmolar or low-osmolar contrast media. Kidney Int. 2006. 70:1811–1817.25. Aspelin P, Aubry P, Fransson SG, Strasser R, Willenbrock R, Berg KJ. Nephrotoxic effects in high-risk patients undergoing angiography. N Engl J Med. 2003. 348:491–499.26. Davidson CJ, Laskey WK, Hermiller JB, et al. Randomized trial of contrast media utilization in high-risk PTCA: the COURT trial. Circulation. 2000. 101:2172–2177.27. Carraro M, Malalan F, Antonione R, et al. Effects of a dimeric vs a monomeric nonionic contrast medium on renal function in patients with mild to moderate renal insufficiency: a double-blind, randomized clinical trial. Eur Radiol. 1998. 8:144–147.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Estimated Glomerular Filtration Rate With Using the Mayo Clinic Quadratic Equation as a New Predictor for Developing Contrast Induced Nephropathy in Patients With Angina Pectoris
- The Efficacy of the Cystatin C Based Glomerular Filtration Rate in the Estimation of Safe Contrast Media Volume
- Effect of High Dose Rosuvastatin Loading before Percutaneous Coronary Intervention on Contrast-Induced Nephropathy
- Contrast Induced Nephropathy and 2-Year Outcomes of Iso-Osmolar Compared with Low-Osmolar Contrast Media after Elective Percutaneous Coronary Intervention
- Successful Treatment of Unprotected Left Main Coronary Bifurcation Lesion Using Minimum Contrast Volume with Intravascular Ultrasound Guidance
