Korean Circ J.
2013 Sep;43(9):622-627. 10.4070/kcj.2013.43.9.622.
The Efficacy of the Cystatin C Based Glomerular Filtration Rate in the Estimation of Safe Contrast Media Volume
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Keimyung University Dongsan Medical Center, Daegu, Korea. khyungseop@dsmc.or.kr
- 2Department of Cardiology, Andong Medical Group, Andong, Korea.
- KMID: 2224818
- DOI: http://doi.org/10.4070/kcj.2013.43.9.622
Abstract
- BACKGROUND AND OBJECTIVES
The risk of contrast-induced nephropathy (CIN) is significantly influenced by baseline renal function and the amount of contrast media (CM). We evaluated the usefulness of the cystatin C (CyC) based estimated glomerular filtration rate (eGFR(CyC)) in the prediction of CIN and to determine the safe CM dosage.
SUBJECTS AND METHODS
We prospectively enrolled a total of 723 patients who received percutaneous coronary intervention (PCI) and investigated the clinical factors associated with the development of CIN. Renal function was calculated as eGFR(CyC) and a modified diet in the renal disease (MDRD) equation, respectively. Systemic exposure of CM was calculated as CM volume to eGFR ratio. We conducted a regression analysis to evaluate the predictive role of CM volume to eGFR(CyC) for the risk of CIN.
RESULTS
The incidence of CIN was 4.0% (29/723). The patients with CIN had a lower hemoglobin level, decreased renal function, and a higher CyC value, and had greater CM exposure. Through multivariate regression analyses, hemoglobin {odds ratio (OR) 0.743, p=0.032}, CM volume/eGFR(CyC) (OR 1.697, p=0.006) and CM volume/MDRD (OR 2.275, p<0.001) were found to be independent predictors for CIN. In the receiver operating characteristic curve analysis, fair discrimination for CIN was found at a CM volume/eGFR(CyC) level of 4.493 (C-statics=0.814), and at this value, the sensitivity and specificity were 79.3% and 80.0%, respectively.
CONCLUSION
Both the CM volume/MDRD and CM volume/eGFR(CyC) method would be simple, useful indicators for determining the safe CM-dose based on eGFR value before PCI. However, there was no significantly different predictive value between creatinine and CyC based GFR estimations.
MeSH Terms
Figure
-
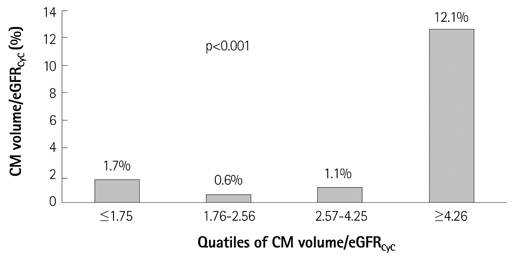
Fig. 1 Incidence of CIN according to the quartiles of CM volume/eGFRCyC. Incidence of CIN is significantly higher in the 4th quartile. CyC: cystatin C, eGFR: estimated glomerular filtration rate.
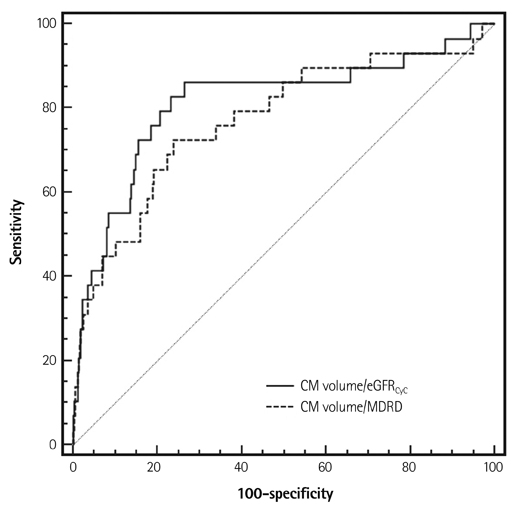
Fig. 2 Receiver operating characteristic curve for the prediction of CIN using CM volume/eGFRCyC and CM volume/MDRD. The area under the curve for predicting CIN of CM volume/eGFRCyC was 0.814 and CM volume/MDRD was 0.772, respectively. CIN: contrast induced nephropathy, CyC: cystatin C, MDRD: equation of modification of diet on renal disease study group.
Reference
-
1. McCullough PA, Wolyn R, Rocher LL, Levin RN, O'Neill WW. Acute renal failure after coronary intervention: incidence, risk factors, and relationship to mortality. Am J Med. 1997; 103:368–375.2. McCullough PA, Adam A, Becker CR, et al. Epidemiology and prognostic implications of contrast-induced nephropathy. Am J Cardiol. 2006; 98:5K–13K.3. Murphy SW, Barrett BJ, Parfrey PS. Contrast nephropathy. J Am Soc Nephrol. 2000; 11:177–182.4. Rihal CS, Textor SC, Grill DE, et al. Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation. 2002; 105:2259–2264.5. Weisbord SD, Mor MK, Resnick AL, et al. Prevention, incidence, and outcomes of contrast-induced acute kidney injury. Arch Intern Med. 2008; 168:1325–1332.6. Mehran R, Aymong ED, Nikolsky E, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. 2004; 44:1393–1399.7. Mehran R, Nikolsky E. Contrast-induced nephropathy: definition, epidemiology, and patients at risk. Kidney Int Suppl. 2006; S11–S15.8. Dangas G, Iakovou I, Nikolsky E, et al. Contrast-induced nephropathy after percutaneous coronary interventions in relation to chronic kidney disease and hemodynamic variables. Am J Cardiol. 2005; 95:13–19.9. Kim U, Kim YJ, Lee WJ, et al. The estimated glomerular filtration rate with using the Mayo clinic quardratic equation as a new predictor for developing contrast induced nephropathy in patients with angina pectoris. Korean Circ J. 2008; 38:301–304.10. Cigarroa RG, Lange RA, Williams RH, Hillis LD. Dosing of contrast material to prevent contrast nephropathy in patients with renal disease. Am J Med. 1989; 86(6 Pt 1):649–652.11. Altmann DB, Zwas D, Spatz A, et al. Use of the contrast volume to estimated creatinine clearance ratio to predict renal failure after angiography. J Interv Cardiol. 1997; 10:113–119.12. Freeman RV, O'Donnell M, Share D, et al. Nephropathy requiring dialysis after percutaneous coronary intervention and the critical role of an adjusted contrast dose. Am J Cardiol. 2002; 90:1068–1073.13. Laskey WK, Jenkins C, Selzer F. Volume-to-creatinine clearance ratio: a pharmacokinetically based risk factor for prediction of early creatinine increase after percutaneous coronary intervention. J Am Coll Cardiol. 2007; 50:584–590.14. Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976; 16:31–41.15. Levey AS, Greene T, Schluchter MD, et al. Glomerular filtration rate measurements in clinical trials. Modification of Diet in Renal Disease Study Group and the Diabetes Control and Complications Trial Research Group. J Am Soc Nephrol. 1993; 4:1159–1171.16. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999; 130:461–470.17. Kyhse-Andersen J, Schmidt C, Nordin G, et al. Serum cystatin C, determined by a rapid, automated particle-enhanced turbidimetric method, is a better marker than serum creatinine for glomerular filtration rate. Clin Chem. 1994; 40:1921–1926.18. Newman DJ, Thakkar H, Edwards RG, et al. Serum cystatin C measured by automated immunoassay: a more sensitive marker of changes in GFR than serum creatinine. Kidney Int. 1995; 47:312–318.19. Dharnidharka VR, Kwon C, Stevens G. Serum cystatin C is superior to serum creatinine as a marker of kidney function: a meta-analysis. Am J Kidney Dis. 2002; 40:221–226.20. Tangri N, Stevens LA, Schmid CH, et al. Changes in dietary protein intake has no effect on serum cystatin C levels independent of the glomerular filtration rate. Kidney Int. 2011; 79:471–477.21. Rule AD, Bergstralh EJ, Slezak JM, Bergert J, Larson TS. Glomerular filtration rate estimated by cystatin C among different clinical presentations. Kidney Int. 2006; 69:399–405.22. Madero M, Sarnak MJ, Stevens LA. Serum cystatin C as a marker of glomerular filtration rate. Curr Opin Nephrol Hypertens. 2006; 15:610–616.23. Perkins BA, Nelson RG, Ostrander BE, et al. Detection of renal function decline in patients with diabetes and normal or elevated GFR by serial measurements of serum cystatin C concentration: results of a 4-year follow-up study. J Am Soc Nephrol. 2005; 16:1404–1412.24. Benko A, Fraser-Hill M, Magner P, et al. Canadian Association of Radiologists: consensus guidelines for the prevention of contrast-induced nephropathy. Can Assoc Radiol J. 2007; 58:79–87.25. Lepanto L, Tang A, Murphy-Lavallée J, Billiard JS. The Canadian Association of Radiologists guidelines for the prevention of contrast-induced nephropathy: a critical appraisal. Can Assoc Radiol J. 2011; 62:238–242.26. Stacul F, van der Molen AJ, Reimer P, et al. Contrast induced nephropathy: updated ESUR Contrast Media Safety Committee guidelines. Eur Radiol. 2011; 21:2527–2541.27. Yoon HJ, Hur SH. Determination of safe contrast media dosage to estimated glomerular filtration rate ratios to avoid contrast-induced nephropathy after elective percutaneous coronary intervention. Korean Circ J. 2011; 41:265–271.28. Hatano M. [Clinical study of tubular creatinine secretion in renal dysfunction]. Nihon Jinzo Gakkai Shi. 1991; 33:1097–1104.29. Chong E, Poh KK, Liang S, Tan HC. Risk factors and clinical outcomes for contrast-induced nephropathy after percutaneous coronary intervention in patients with normal serum creatinine. Ann Acad Med Singapore. 2010; 39:374–380.30. Lee KH, Lee SR, Kang KP, et al. Periprocedural hemoglobin drop and contrast-induced nephropathy in percutaneous coronary intervention patients. Korean Circ J. 2010; 40:68–73.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Value of Serum Concentration of Cystatin C as a Marker for Glomerular Filtration Rate in Children and Adolescents
- Reference Values for Cystatin C Serum Concentrations in Children
- Serum Cystatin C Compared with Other Markers for Glomerular Filtration Rate
- Cystatin C as a Marker for Early Renal Impairment
- Relationship between serum cystatin C and glomerular filtration rate in renal transplant patients
