Benign Paroxysmal Positional Vertigo
- Affiliations
-
- 1Department of Neurology, Chonnam National University Medical School, Gwangju, Korea.
- 2Department of Neurology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea. jisookim@snu.ac.kr
- 3Department of Neurology, Johns Hopkins University School of Medicine, Baltimore, USA.
- KMID: 2287635
- DOI: http://doi.org/10.3988/jcn.2010.6.2.51
Abstract
- Benign paroxysmal positional vertigo (BPPV) is characterized by brief recurrent episodes of vertigo triggered by changes in head position. BPPV is the most common etiology of recurrent vertigo and is caused by abnormal stimulation of the cupula by free-floating otoliths (canalolithiasis) or otoliths that have adhered to the cupula (cupulolithiasis) within any of the three semicircular canals. Typical symptoms and signs of BPPV are evoked when the head is positioned so that the plane of the affected semicircular canal is spatially vertical and thus aligned with gravity. Paroxysm of vertigo and nystagmus develops after a brief latency during the Dix-Hallpike maneuver in posterior-canal BPPV, and during the supine roll test in horizontal-canal BPPV. Positioning the head in the opposite direction usually reverses the direction of the nystagmus. The duration, frequency, and symptom intensity of BPPV vary depending on the involved canals and the location of otolithic debris. Spontaneous recovery may be expected even with conservative treatments. However, canalithrepositioning maneuvers usually provide an immediate resolution of symptoms by clearing the canaliths from the semicircular canal into the vestibule.
Figure
-
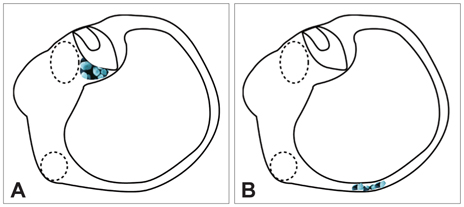
Fig. 1 Mechanism of benign paroxysmal positional vertigo (BPPV). The detached otolith debris may be attached to the cupula (A: Cupulolithiasis) or free-floating in the semicircular canals (B: Canalolithiasis).
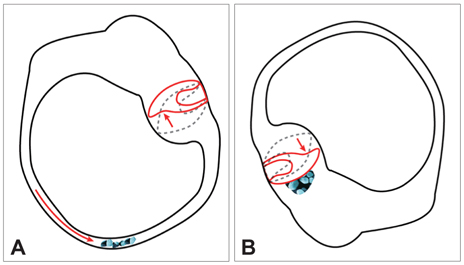
Fig. 2 Deflection of the cupula due to either endolymphatic flow induced by a hydrodynamic drag of the particles (A: Canalolithiasis) or a direct gravitational effect of the otolithic debris (B: Cupulolithiasis).

Fig. 3 Dix-Hallpike maneuver for the diagnosis of BPPV involving the right posterior semicircular canal (right PC-BPPV). After seating the patient upright (A), the head is turned 45° in the direction of the involved ear (B: right ear in this figure). The patient is then moved from the sitting to the supine position, ending with the head hanging at 20° off the end of the examination table (C). The corresponding illustrations demonstrate the orientation of the semicircular canals and location of the otolithic debris in the posterior canal (viewed from the patient's right side). BPPV: benign paroxysmal positional vertigo.

Fig. 4 Side-lying test for the diagnosis of right PC-BPPV. After seating the patient on the examination table (A), the head is turned 45° away from the involved ear (B). The patient then lies on the side of the involved ear (C). The corresponding illustrations demonstrate the orientation of the semicircular canals and location of the otolithic debris in the posterior canal (viewed from the front). PC-BPPV: posterior canal benign paroxysmal positional vertigo.
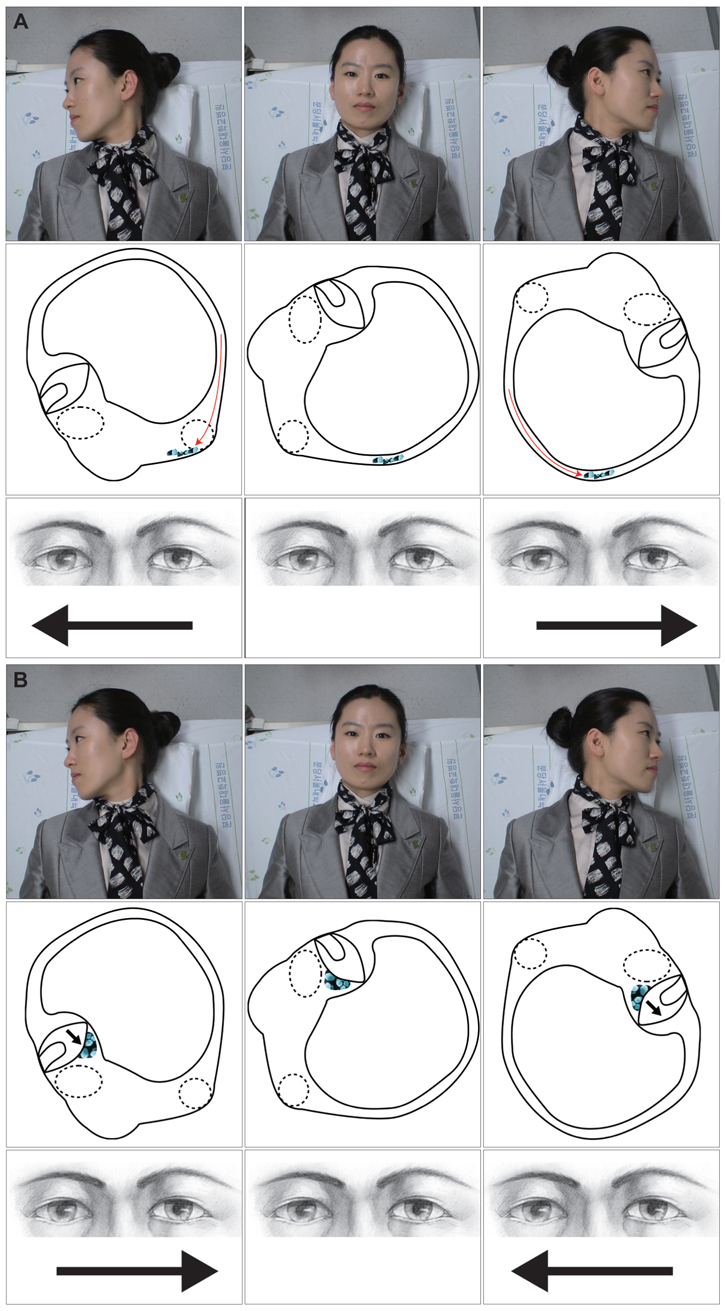
Fig. 5 Supine roll test (Pagnini-McClure maneuver) for the diagnosis of BPPV involving the horizontal semicircular canal (right HC-BPPV). The head is turned about 90° to each side while supine. A: Canalolithiasis. B: Cupulolithiasis. The corresponding illustrations demonstrate the location of the otolithic debris in the horizontal canal during each maneuver, and the direction of the induced nystagmus (arrows). BPPV: benign paroxysmal positional vertigo.
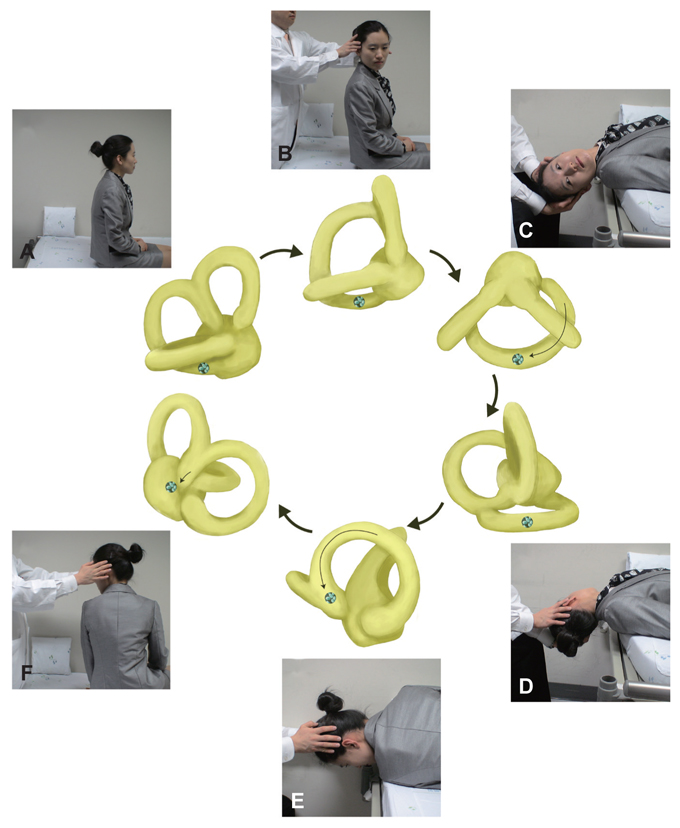
Fig. 6 Modified Epley's maneuver for the treatment of right PC-BPPV. After the Dix-Hallpike maneuver (A-C) for right PC-BPPV, the head is turned 90° toward the unaffected ear (D) and the head and trunk continue turning another 90° in the same direction (E). The patient is then moved to the sitting position (F). Each position should be maintained for at least 1 or 2 minutes, or until the induced nystagmus and vertigo are resolved. The corresponding illustrations demonstrate the orientation of the semicircular canals and location of the otolithic debris in the posterior canal (viewed from the camera angle). PC-BPPV: posterior canal benign paroxysmal positional vertigo.
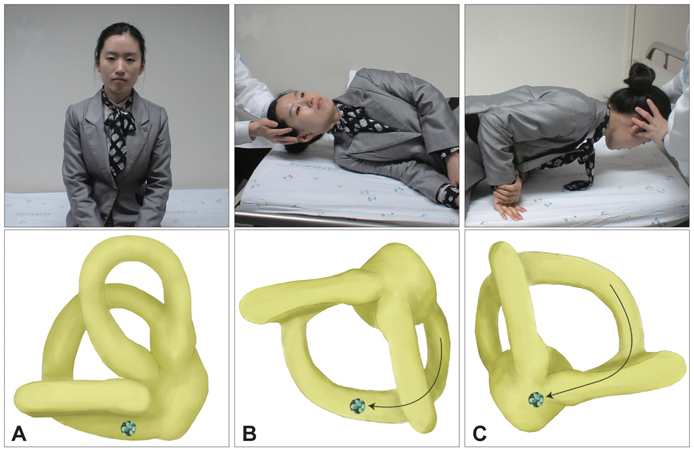
Fig. 7 Semont maneuver for the treatment of right PC-BPPV. After being seated on the examination table (A), the patient is rapidly moved into the side-lying position to the affected side after the head is turned 45° to the unaffected side (B). The patient is then rapidly taken to the opposite side-lying position through the seated position without pausing (C). The head should be rotated toward the unaffected side throughout these movements. Finally, the patient is returned to a seated position. Each position should be maintained for at least 1 or 2 minutes, or until the induced nystagmus and vertigo are resolved. The corresponding illustrations demonstrate the orientation of the semicircular canals and location of the otolithic debris in the posterior canal (viewed from the camera angle). PC-BPPV: posterior canal benign paroxysmal positional vertigo.
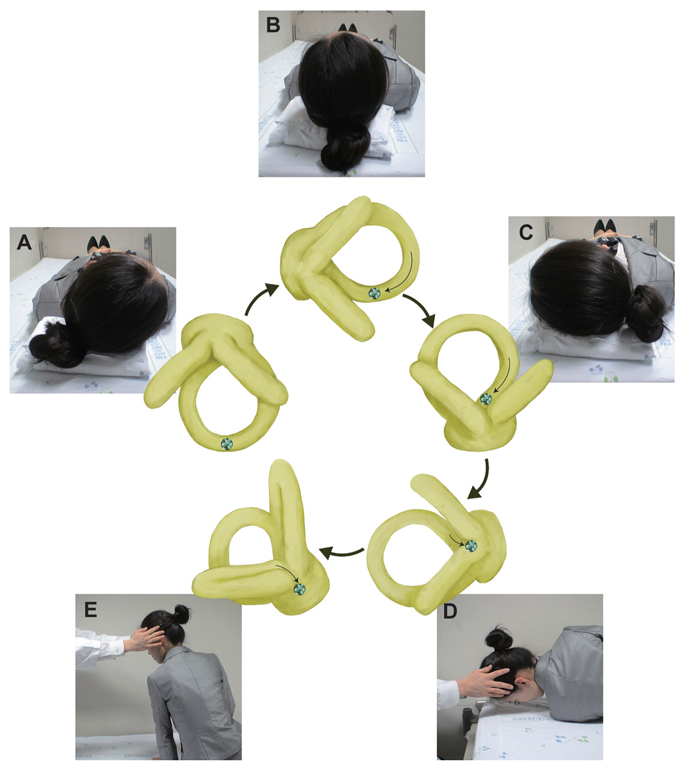
Fig. 8 Barbecue maneuver for the treatment of geotropic right HC-BPPV. After head turning toward the involved ear (A), the head is then turned 270° toward the unaffected side through a series of stepwise 90° turns (B-D) before resuming the sitting position (E). Each position should be maintained for at least 1 or 2 minutes, or until the induced nystagmus and vertigo are resolved. The corresponding illustrations demonstrate the orientation of the semicircular canals and the location of the otolithic debris in the horizontal canal. HC-BPPV: horizontal canal benign paroxysmal positional positional vertigo.

Fig. 9 Brandt-Daroff exercise. Patients are instructed to rapidly lie on their side, sit up, lie on the opposite side, and then again sit up. Each position should be maintained for at least 30 seconds. These exercises are repeated serially 5-10 times a day until resolution of the symptoms.
Cited by 2 articles
-
Clinical approach to patients with dizziness
Jae Han Park, Youngrok Do, Ji Soo Kim
J Korean Med Assoc. 2018;61(1):44-48. doi: 10.5124/jkma.2018.61.1.44.Persistent Direction-Fixed Nystagmus Following Canalith Repositioning Maneuver for Horizontal Canal BPPV: A Case of Canalith Jam
Young-Soo Chang, Jeesun Choi, Won-Ho Chung
Clin Exp Otorhinolaryngol. 2014;7(2):138-141. doi: 10.3342/ceo.2014.7.2.138.
Reference
-
1. Hotson JR, Baloh RW. Acute vestibular syndrome. N Engl J Med. 1998. 339:680–685.
Article2. Furman JM, Cass SP. Benign paroxysmal positional vertigo. N Engl J Med. 1999. 341:1590–1596.
Article3. Bertholon P, Tringali S, Faye MB, Antoine JC, Martin C. Prospective study of positional nystagmus in 100 consecutive patients. Ann Otol Rhinol Laryngol. 2006. 115:587–594.
Article4. Steenerson RL, Cronin GW, Marbach PM. Effectiveness of treatment techniques in 923 cases of benign paroxysmal positional vertigo. Laryngoscope. 2005. 115:226–231.
Article5. Barany R. Diagnose von krankheitserscheinungen im. Bereiche des otolithenapparates. Acta Otolaryngol. 1921. 2:434–437.6. Dix MR, Hallpike CS. The pathology symptomatology and diagnosis of certain common disorders of the vestibular system. Proc R Soc Med. 1952. 45:341–354.
Article7. Schuknecht HF. Cupulolithiasis. Arch Otolaryngol. 1969. 90:765–778.
Article8. Hall SF, Ruby RR, McClure JA. The mechanics of benign paroxysmal vertigo. J Otolaryngol. 1979. 8:151–158.9. Parnes LS, McClure JA. Free-floating endolymph particles: a new operative finding during posterior semicircular canal occlusion. Laryngoscope. 1992. 102:988–992.10. Semont A, Freyss G, Vitte E. Curing the BPPV with a liberatory maneuver. Adv Otorhinolaryngol. 1988. 42:290–293.
Article11. Epley JM. The canalith repositioning procedure: for treatment of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg. 1992. 107:399–404.
Article12. McClure JA. Horizontal canal BPV. J Otolaryngol. 1985. 14:30–35.13. Baloh RW, Yue Q, Jacobson KM, Honrubia V. Persistent direction-changing positional nystagmus: another variant of benign positional nystagmus? Neurology. 1995. 45:1297–1301.
Article14. Honrubia V, Baloh RW, Harris MR, Jacobson KM. Paroxysmal positional vertigo syndrome. Am J Otol. 1999. 20:465–470.15. Schratzenstaller B, Wagner-Manslau C, Strasser G, Arnold W. Canalolithiasis of the superior semicircular canal: an anomaly in benign paroxysmal vertigo. Acta Otolaryngol. 2005. 125:1055–1062.
Article16. Blatt PJ, Georgakakis GA, Herdman SJ, Clendaniel RA, Tusa RJ. The effect of the canalith repositioning maneuver on resolving postural instability in patients with benign paroxysmal positional vertigo. Am J Otol. 2000. 21:356–363.
Article17. Giacomini PG, Alessandrini M, Magrini A. Long-term postural abnormalities in benign paroxysmal positional vertigo. ORL J Otorhinolaryngol Relat Spec. 2002. 64:237–241.
Article18. Baloh RW, Jacobson K, Honrubia V. Horizontal semicircular canal variant of benign positional vertigo. Neurology. 1993. 43:2542–2549.
Article19. Bhattacharyya N, Baugh RF, Orvidas L, Barrs D, Bronston LJ, Cass S, et al. Clinical practice guideline: benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg. 2008. 139:S47–S81.
Article20. von Brevern M, Radtke A, Lezius F, Feldmann M, Ziese T, Lempert T, et al. Epidemiology of benign paroxysmal positional vertigo: a population based study. J Neurol Neurosurg Psychiatry. 2007. 78:710–715.
Article21. Baloh RW, Honrubia V, Jacobson K. Benign positional vertigo: clinical and oculographic features in 240 cases. Neurology. 1987. 37:371–378.
Article22. von Brevern M, Seelig T, Neuhauser H, Lempert T. Benign paroxysmal positional vertigo predominantly affects the right labyrinth. J Neurol Neurosurg Psychiatry. 2004. 75:1487–1488.
Article23. Parnes LS, Agrawal SK, Atlas J. Diagnosis and management of benign paroxysmal positional vertigo (BPPV). CMAJ. 2003. 169:681–693.24. Moon SY, Kim JS, Kim BK, Kim JI, Lee H, Son SI, et al. Clinical characteristics of benign paroxysmal positional vertigo in Korea: a multicenter study. J Korean Med Sci. 2006. 21:539–543.
Article25. Nuti D, Mandalà M, Salerni L. Lateral canal paroxysmal positional vertigo revisited. Ann N Y Acad Sci. 2009. 1164:316–323.
Article26. Imai T, Ito M, Takeda N, Uno A, Matsunaga T, Sekine K, et al. Natural course of the remission of vertigo in patients with benign paroxysmal positional vertigo. Neurology. 2005. 64:920–921.
Article27. De la Meilleure G, Dehaene I, Depondt M, Damman W, Crevits L, Vanhooren G. Benign paroxysmal positional vertigo of the horizontal canal. J Neurol Neurosurg Psychiatry. 1996. 60:68–71.
Article28. Vibert D, Kompis M, Häusler R. Benign paroxysmal positional vertigo in older women may be related to osteoporosis and osteopenia. Ann Otol Rhinol Laryngol. 2003. 112:885–889.
Article29. Jeong SH, Choi SH, Kim JY, Koo JW, Kim HJ, Kim JS. Osteopenia and osteoporosis in idiopathic benign positional vertigo. Neurology. 2009. 72:1069–1076.
Article30. Karlberg M, Hall K, Quickert N, Hinson J, Halmagyi GM. What inner ear diseases cause benign paroxysmal positional vertigo? Acta Otolaryngol. 2000. 120:380–385.
Article31. Gordon CR, Levite R, Joffe V, Gadoth N. Is posttraumatic benign paroxysmal positional vertigo different from the idiopathic form? Arch Neurol. 2004. 61:1590–1593.
Article32. Katsarkas A. Benign paroxysmal positional vertigo (BPPV): idiopathic versus post-traumatic. Acta Otolaryngol. 1999. 119:745–749.
Article33. Hong SL, Kim JS, Koo JW. A case of contralateral benign paroxysmal positional vertigo after mastoidectomy. J Korean Bal Soc. 2005. 4:45–48.34. Kaplan DM, Attal U, Kraus M. Bilateral benign paroxysmal positional vertigo following a tooth implantation. J Laryngol Otol. 2003. 117:312–313.
Article35. Ishiyama A, Jacobson KM, Baloh RW. Migraine and benign positional vertigo. Ann Otol Rhinol Laryngol. 2000. 109:377–380.
Article36. Cohen HS, Kimball KT, Stewart MG. Benign paroxysmal positional vertigo and comorbid conditions. ORL J Otorhinolaryngol Relat Spec. 2004. 66:11–15.
Article37. Ziavra NV, Bronstein AM. Is uric acid implicated in benign paroxysmal positional vertigo? J Neurol. 2004. 251:115.
Article38. Amor-Dorado JC, Llorca J, Costa-Ribas C, Garcia-Porrua C, Gonzalez-Gay MA. Giant cell arteritis: a new association with benign paroxysmal positional vertigo. Laryngoscope. 2004. 114:1420–1425.
Article39. von Brevern M, Schmidt T, Schönfeld U, Lempert T, Clarke AH. Utricular dysfunction in patients with benign paroxysmal positional vertigo. Otol Neurotol. 2006. 27:92–96.
Article40. Ushio M, Murofushi T, Iwasaki S. Subjective visual horizontal in patients with posterior canal benign paroxysmal positional vertigo. Acta Otolaryngol. 2007. 127:836–838.
Article41. Yang WS, Kim SH, Lee JD, Lee WS. Clinical significance of vestibular evoked myogenic potentials in benign paroxysmal positional vertigo. Otol Neurotol. 2008. 29:1162–1166.
Article42. Sugita-Kitajima A, Koizuka I. Recovery of otolith function in patients with benign paroxysmal positional vertigo evaluated by sinusoidal off-vertical axis rotation. Neurosci Lett. 2008. 436:124–127.
Article43. Otsuka K, Suzuki M, Furuya M. Model experiment of benign paroxysmal positional vertigo mechanism using the whole membranous labyrinth. Acta Otolaryngol. 2003. 123:515–518.
Article44. Humphriss RL, Baguley DM, Sparkes V, Peerman SE, Moffat DA. Contraindications to the Dix-Hallpike manoeuvre: a multidisciplinary review. Int J Audiol. 2003. 42:166–173.
Article45. Asprella Libonati G. Diagnostic and treatment strategy of lateral semicircular canal canalolithiasis. Acta Otorhinolaryngol Ital. 2005. 25:277–283.46. Han BI, Oh HJ, Kim JS. Nystagmus while recumbent in horizontal canal benign paroxysmal positional vertigo. Neurology. 2006. 66:706–710.
Article47. Koo JW, Moon IJ, Shim WS, Moon SY, Kim JS. Value of lying-down nystagmus in the lateralization of horizontal semicircular canal benign paroxysmal positional vertigo. Otol Neurotol. 2006. 27:367–371.
Article48. Lee SH, Choi KD, Jeong SH, Oh YM, Koo JW, Kim JS. Nystagmus during neck flexion in the pitch plane in benign paroxysmal positional vertigo involving the horizontal canal. J Neurol Sci. 2007. 256:75–80.
Article49. Bisdorff AR, Debatisse D. Localizing signs in positional vertigo due to lateral canal cupulolithiasis. Neurology. 2001. 57:1085–1088.
Article50. Asprella-Libonati G. Pseudo-spontaneous nystagmus: a new sign to diagnose the affected side in lateral semicircular canal benign paroxysmal positional vertigo. Acta Otorhinolaryngol Ital. 2008. 28:73–78.51. von Brevern M, Clarke AH, Lempert T. Continuous vertigo and spontaneous nystagmus due to canalolithiasis of the horizontal canal. Neurology. 2001. 56:684–686.
Article52. Lee SH, Kim MK, Cho KH, Kim JS. Reversal of initial positioning nystagmus in benign paroxysmal positional vertigo involving the horizontal canal. Ann N Y Acad Sci. 2009. 1164:406–408.
Article53. Brantberg K, Bergenius J. Treatment of anterior benign paroxysmal positional vertigo by canal plugging: a case report. Acta Otolaryngol. 2002. 122:28–30.
Article54. Zapala DA. Down-beating nystagmus in anterior canal benign paroxysmal positional vertigo. J Am Acad Audiol. 2008. 19:257–266.
Article55. Tomaz A, Ganança MM, Ganança CF, Ganança FF, Caovilla HH, Harker L. Benign paroxysmal positional vertigo: concomitant involvement of different semicircular canals. Ann Otol Rhinol Laryngol. 2009. 118:113–117.
Article56. Arai M, Terakawa I. Central paroxysmal positional vertigo. Neurology. 2005. 64:1284.
Article57. Kattah JC, Talkad AV, Wang DZ, Hsieh YH, Newman-Toker DE. HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke. 2009. 40:3504–3510.
Article58. Bertholon P, Bronstein AM, Davies RA, Rudge P, Thilo KV. Positional down beating nystagmus in 50 patients: cerebellar disorders and possible anterior semicircular canalithiasis. J Neurol Neurosurg Psychiatry. 2002. 72:366–372.
Article59. Nam J, Kim S, Huh Y, Kim JS. Ageotropic central positional nystagmus in nodular infarction. Neurology. 2009. 73:1163.
Article60. Anagnostou E, Mandellos D, Limbitaki G, Papadimitriou A, Anastasopoulos D. Positional nystagmus and vertigo due to a solitary brachium conjunctivum plaque. J Neurol Neurosurg Psychiatry. 2006. 77:790–792.
Article61. Seok JI, Lee HM, Yoo JH, Lee DK. Residual dizziness after successful repositioning treatment in patients with benign paroxysmal positional vertigo. J Clin Neurol. 2008. 4:107–110.
Article62. Brandt T, Daroff RB. Physical therapy for benign paroxysmal positional vertigo. Arch Otolaryngol. 1980. 106:484–485.
Article63. Sargent EW, Bankaitis AE, Hollenbeak CS, Currens JW. Mastoid oscillation in canalith repositioning for paroxysmal positional vertigo. Otol Neurotol. 2001. 22:205–209.
Article64. Macias JD, Ellensohn A, Massingale S, Gerkin R. Vibration with the canalith repositioning maneuver: a prospective randomized study to determine efficacy. Laryngoscope. 2004. 114:1011–1014.
Article65. Casqueiro JC, Ayala A, Monedero G. No more postural restrictions in posterior canal benign paroxysmal positional vertigo. Otol Neurotol. 2008. 29:706–709.
Article66. Hilton M, Pinder D. The Epley (canalith repositioning) manoeuvre for benign paroxysmal positional vertigo. Cochrane Database Syst Rev. 2004. CD003162.
Article67. Oh HJ, Kim JS, Han BI, Lim JG. Predicting a successful treatment in posterior canal benign paroxysmal positional vertigo. Neurology. 2007. 68:1219–1222.
Article68. Fife TD, Iverson DJ, Lempert T, Furman JM, Baloh RW, Tusa RJ, et al. Practice parameter: therapies for benign paroxysmal positional vertigo (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2008. 70:2067–2074.
Article69. Salvinelli F, Trivelli M, Casale M, Firrisi L, Di Peco V, D'Ascanio L, et al. Treatment of benign positional vertigo in the elderly: a randomized trial. Laryngoscope. 2004. 114:827–831.
Article70. Radtke A, Neuhauser H, von Brevern M, Lempert T. A modified Epley's procedure for self-treatment of benign paroxysmal positional vertigo. Neurology. 1999. 53:1358–1360.
Article71. Radtke A, von Brevern M, Tiel-Wilck K, Mainz-Perchalla A, Neuhauser H, Lempert T. Self-treatment of benign paroxysmal positional vertigo: Semont maneuver vs Epley procedure. Neurology. 2004. 63:150–152.
Article72. Lempert T. Horizontal benign positional vertigo. Neurology. 1994. 44:2213–2214.
Article73. Vannucchi P, Giannoni B, Pagnini P. Treatment of horizontal semicircular canal benign paroxysmal positional vertigo. J Vestib Res. 1997. 7:1–6.
Article74. Appiani GC, Catania G, Gagliardi M. A liberatory maneuver for the treatment of horizontal canal paroxysmal positional vertigo. Otol Neurotol. 2001. 22:66–69.
Article75. [Repositioning maneuver in benign paroxysmal vertigo of horizontal semicircular canal]. Acta Otorhinolaryngol Ital. 1998. 18:363–367.76. Riggio F, Dispenza F, Gallina S, Kulamarva G, Gargano R, Speciale R. Management of benign paroxysmal positional vertigo of lateral semicircular canal by Gufoni's manoeuvre. Am J Otolaryngol. 2009. 30:106–111.
Article77. Oh SY, Kim JS, Jeong SH, Oh YM, Choi KD, Kim BK, et al. Treatment of apogeotropic benign positional vertigo: comparison of therapeutic head-shaking and modified Semont maneuver. J Neurol. 2009. 256:1330–1336.
Article78. Nuti D, Vannucchi P, Pagnini P. Benign paroxysmal positional vertigo of the horizontal canal: a form of canalolithiasis with variable clinical features. J Vestib Res. 1996. 6:173–184.
Article79. Casani AP, Vannucci G, Fattori B, Berrettini S. The treatment of horizontal canal positional vertigo: our experience in 66 cases. Laryngoscope. 2002. 112:172–178.
Article80. Appiani GC, Catania G, Gagliardi M, Cuiuli G. Repositioning maneuver for the treatment of the apogeotropic variant of horizontal canal benign paroxysmal positional vertigo. Otol Neurotol. 2005. 26:257–260.
Article81. Crevits L. Treatment of anterior canal benign paroxysmal positional vertigo by a prolonged forced position procedure. J Neurol Neurosurg Psychiatry. 2004. 75:779–781.
Article82. Kim YK, Shin JE, Chung JW. The effect of canalith repositioning for anterior semicircular canal canalithiasis. ORL J Otorhinolaryngol Relat Spec. 2005. 67:56–60.
Article83. Norré ME. Rationale of rehabilitation treatment for vertigo. Am J Otolaryngol. 1987. 8:31–35.
Article84. Leveque M, Labrousse M, Seidermann L, Chays A. Surgical therapy in intractable benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg. 2007. 136:693–698.
Article85. Agrawal SK, Parnes LS. Human experience with canal plugging. Ann N Y Acad Sci. 2001. 942:300–305.
Article86. Pournaras I, Kos I, Guyot JP. Benign paroxysmal positional vertigo: a series of eight singular neurectomies. Acta Otolaryngol. 2008. 128:5–8.
Article87. Gacek RR. Transection of the posterior ampullary nerve for the relief of benign paroxysmal positional vertigo. Ann Otol Rhinol Laryngol. 1974. 83:596–605.
Article88. Hain TC, Uddin M. Pharmacological treatment of vertigo. CNS Drugs. 2003. 17:85–100.
Article89. Fujino A, Tokumasu K, Yosio S, Naganuma H, Yoneda S, Nakamura K. Vestibular training for benign paroxysmal positional vertigo. Its efficacy in comparison with antivertigo drugs. Arch Otolaryngol Head Neck Surg. 1994. 120:497–504.
Article90. Brandt T, Zwergal A, Strupp M. Medical treatment of vestibular disorders. Expert Opin Pharmacother. 2009. 10:1537–1548.
Article91. Del Rio M, Arriaga MA. Benign positional vertigo: prognostic factors. Otolaryngol Head Neck Surg. 2004. 130:426–429.
Article92. Sakaida M, Takeuchi K, Ishinaga H, Adachi M, Majima Y. Long-term outcome of benign paroxysmal positional vertigo. Neurology. 2003. 60:1532–1534.
Article93. Brandt T, Huppert D, Hecht J, Karch C, Strupp M. Benign paroxysmal positioning vertigo: a long-term follow-up (6-17 years) of 125 patients. Acta Otolaryngol. 2006. 126:160–163.
Article94. Li JC, Li CJ, Epley J, Weinberg L. Cost-effective management of benign positional vertigo using canalith repositioning. Otolaryngol Head Neck Surg. 2000. 122:334–339.
Article95. Bergenius J, Tomanovic T. Persistent geotropic nystagmus--a different kind of cupular pathology and its localizing signs. Acta Otolaryngol. 2006. 126:698–704.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Positional Dizziness and Vertigo without Nystagmus and Orthostatic Hypotension
- Diagnosis of Benign Paroxysmal Positional Vertigo
- Model Experiment of Benign Paroxysmal Positional Vertigo
- Vestibular Paroxysmia Mimicking Benign Parxysmal Positional Vertigo
- The History of Research in Vestibular Organ and Benign Paroxysmal Positional Vertigo
