Allergy Asthma Respir Dis.
2014 Jul;2(3):213-217. 10.4168/aard.2014.2.3.213.
Cefepime-induced encephalopathy without renal impairment
- Affiliations
-
- 1Department of Internal Medicine, Dong-A University College of Medicine, Busan, Korea. skleeai@dau.ac.kr
- 2Dong-A University Hospital Regional Pharmacovigilance Center, Busan, Korea.
- 3Department of Pharmacy, Dong-A University Hospital, Busan, Korea.
- KMID: 2262522
- DOI: http://doi.org/10.4168/aard.2014.2.3.213
Abstract
- Cefepime is an extended-spectrum, fourth-generation cephalosporin that has been widely used for approved indications such as febrile neutropenia. Common adverse events of cefepime include headache, skin rash, gastrointestinal problems, and fever. However, encephalopathathy caused by cefepime has been sporadically reported worldwide over the last decade. We experienced a rare case of cefepime-induced encephalopathy. A 75-year-old man with a 30-year history of chronic obstructive pulmonary disease was admitted to the medical intensive care unit under a diagnosis of pneumonia. Initial antibiotic therapy was started with piperacillin/sulbactam and ciprofloxacin. His condition was improved with this treatment. About 2 months later, his condition was aggravated again, with mild fever and purulent sputum. Intravenous cefepime was selected on the basis of antibiotic susceptibility to Pseudomonas aeruginosa isolated from his sputum. However, his mentality became drowsy 48 hours after cefepime adminstration. He showed tremors and right facial paralysis. Neurologic examination for motor power and sensory function revealed normal findings. Laboratory tests, including serum electrolytes, glucose, osmolality, and ammonia, gave normal results. Brain magnetic resonance imaging showed chronic ischemic and atropic changes, and an electroencephalography revealed triphasic waves. The administration of cefepime was stopped, and his symptoms started to improve within 48 hours. Electroencephalography results became normalized, and he completely recovered within 48 hours after discontinuation of cefepime.
MeSH Terms
-
Aged
Ammonia
Brain
Ciprofloxacin
Diagnosis
Electroencephalography
Electrolytes
Exanthema
Facial Paralysis
Febrile Neutropenia
Fever
Glucose
Headache
Humans
Intensive Care Units
Magnetic Resonance Imaging
Nervous System Diseases
Neurologic Examination
Osmolar Concentration
Pneumonia
Pseudomonas aeruginosa
Pulmonary Disease, Chronic Obstructive
Sensation
Sputum
Tremor
Ammonia
Ciprofloxacin
Electrolytes
Glucose
Figure
-
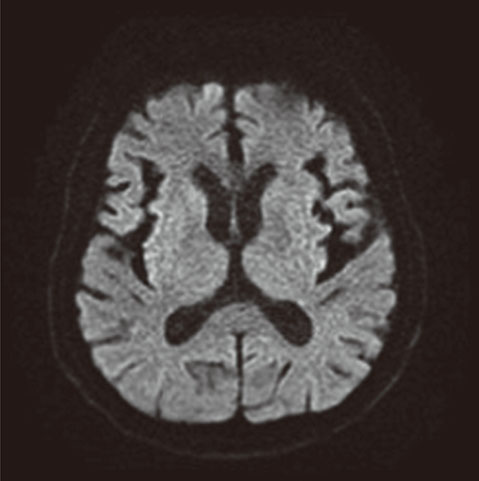
Fig. 1 Brain magnetic resonance imaging shows chronic ischemic and atropic changes.

Fig. 2 The initial electroencephalography showed the triphasic nonconvulsive ictal wave (A), and the electroencephalography became normal shape without triphasic wave after discontinuance of cefepime (B). The green square box indicates triphasic ictal wave in frontal lobe.
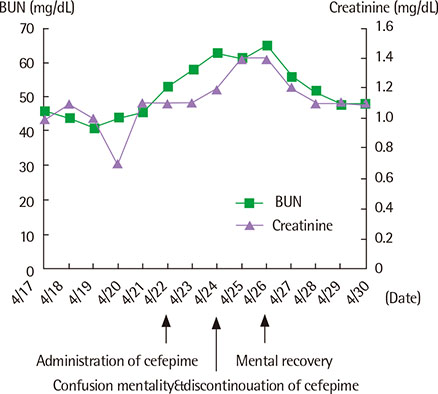
Fig. 3 The change of blood urea nitrogen (BUN) and creatinine during hospital admissions was presented.
Cited by 1 articles
-
Cefepime-induced neurotoxicity
Se-Jin Lee
J Neurocrit Care. 2019;12(2):74-84. doi: 10.18700/jnc.190109.
Reference
-
1. Yahav D, Paul M, Fraser A, Sarid N, Leibovici L. Efficacy and safety of cefepime: a systematic review and meta-analysis. Lancet Infect Dis. 2007; 7:338–348.
Article2. Bragatti JA. Cefepime-induced neurotoxicity. Cent Nerv Syst Agents Med Chem. 2008; 8:229–233.
Article3. Jallon P, Fankhauser L, Du Pasquier R, Coeytaux A, Picard F, Hefft S, et al. Severe but reversible encephalopathy associated with cefepime. Neurophysiol Clin. 2000; 30:383–386.
Article4. Ryu JA, Lee SM, Kim JI, Lee GH, Lee CM, Song YM, et al. Cefepime-induced reversible encephalopathy with triphasic waves in patients with impaired renal function. J Korean Epilepsy Soc. 2009; 13:15–18.5. Baek SD, Park SJ, Baek CH, Koo TY, Kang JK, Kim SB. Neurotoxicity induced by cefepime in a patient with minimal change disease. Korean J Nephrol. 2010; 29:796–801.6. Gilbert DN, Moellering RC, Eliopoulos GM, Chambers HF, Saag MS, editors. The Sanford guide to antimicrobial therapy. 43th ed. Sperryville, VA: Antimicrobial Therapy;2013.7. Sonck J, Laureys G, Verbeelen D. The neurotoxicity and safety of treatment with cefepime in patients with renal failure. Nephrol Dial Transplant. 2008; 23:966–970.
Article8. Chow KM, Szeto CC, Hui AC, Wong TY, Li PK. Retrospective review of neurotoxicity induced by cefepime and ceftazidime. Pharmacotherapy. 2003; 23:369–373.
Article9. Barbhaiya RH, Knupp CA, Forgue ST, Matzke GR, Guay DR, Pittman KA. Pharmacokinetics of cefepime in subjects with renal insufficiency. Clin Pharmacol Ther. 1990; 48:268–276.
Article10. Lamoth F, Buclin T, Pascual A, Vora S, Bolay S, Decosterd LA, et al. High cefepime plasma concentrations and neurological toxicity in febrile neutropenic patients with mild impairment of renal function. Antimicrob Agents Chemother. 2010; 54:4360–4367.
Article11. Sugimoto M, Uchida I, Mashimo T, Yamazaki S, Hatano K, Ikeda F, et al. Evidence for the involvement of GABA(A) receptor blockade in convulsions induced by cephalosporins. Neuropharmacology. 2003; 45:304–314.
Article12. Yang Y, Rosenberg GA. Blood-brain barrier breakdown in acute and chronic cerebrovascular disease. Stroke. 2011; 42:3323–3328.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cefepime-Induced Reversible Encephalopathy with Triphasic Waves in Patients with Impaired Renal Function
- Cefepime Induced Encephalopathy Mimicking Acute Stroke
- Cefepime-induced neurotoxicity
- Cefepime Neurotoxicity in Patients with Renal Insufficiency
- Neurotoxicity Induced by Cefepime in a Patient with Minimal Change Disease
