A Retrospective Study on the Efficacy of a Ten-Milligram Dosage of Atorvastatin for Treatment of Hypercholesterolemia in Type 2 Diabetes Mellitus Patients
- Affiliations
-
- 1Department of Internal Medicine, Dong-A University Medical Center, Dong-A University College of Medicine, Busan, Korea. dkkim@dau.ac.kr
- 2Department of Pharmacology, Dong-A University Medical Center, Dong-A University College of Medicine, Busan, Korea.
- 3Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2222363
- DOI: http://doi.org/10.4093/kdj.2010.34.6.359
Abstract
- BACKGROUND
There have been few clinical studies on 10 mg atorvastatin as a starting dosage for treatment of hypercholesterolemia in type 2 diabetes mellitus (T2DM) patients. This retrospective study aims to evaluate the efficacy of 10 mg dosage of atorvastatin in clinical setting.
METHODS
One hundred five enrolled patients with high levels of low density lipoprotein cholesterol (LDL-C, > 100 mg/dL) took 10 mg atorvastatin. After 6 months, they were divided into 'Responder group' (LDL-C < 100 mg/dL) and 'Non-responder group' (LDL-C > or = 100 mg/dL), and the response rate was calculated. Thereafter, we subdivided the 'Responder group' into Maintenance (10 mg), Reduced dosage (5 mg), and Discontinuance group (0 mg). The 'Non-Responder group' was subdivided into Maintenance (10 mg) and Double dosage group (20 mg). After consecutive 6 months, the response rates of each 10 mg Maintenance groups were compared to those of the other groups, respectively.
RESULTS
Following the first 6 months, the response rate of 10 mg fixed dosage was 74.3%. In the 'Responder group', response rates of 10 mg, 5 mg and Discontinuance groups following 6 months were 52.6%, 53.1%, and 12.5%, respectively. In the 'Non-responder group', response rates of 10 mg and 20 mg groups were 28.6% and 50.0%. Baseline LDL-C levels and body mass index (BMI) of 'Responder group' were significantly lower than those of 'Non-responder group' (P = 0.004, respectively).
CONCLUSION
Hypercholesterolemia treatment with 10 mg, fixed dosage of atorvastatin was effective in three quarters of the subjects during the first 6-month treatment; however, a significant number of patients with high LDL-C levels and/or BMI require higher starting and maintenance dosage.
MeSH Terms
Figure
-
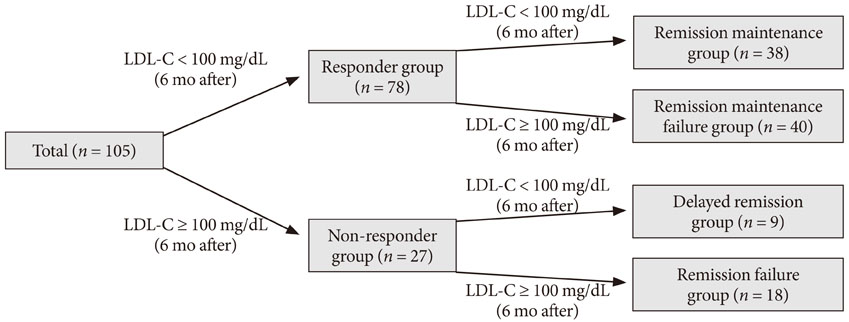
Fig. 1 Schematic flow diagram of study setting: 105 patients with type 2 diabetes mellitus (T2DM) underwent atorvastatin 10 mg therapy as starting dose for reducing high low density lipoprotein cholesterol (LDL-C) levels (> 100 mg/dL) were enrolled for the study. After 6 months of treatment, the subjects were divided into a responder group (LDL-C < 100 mg/dL) or Non-Responder group (LDL-C ≥ 100 mg/dL). Thereafter, the Responder group was subdivided into a Remission maintenance group and Remission maintenance failure group. The Non-responder group was subdivided into a Delayed remission group and Remission failure group. Dosage modifications were made following a response to each dosage of atorvastatin.
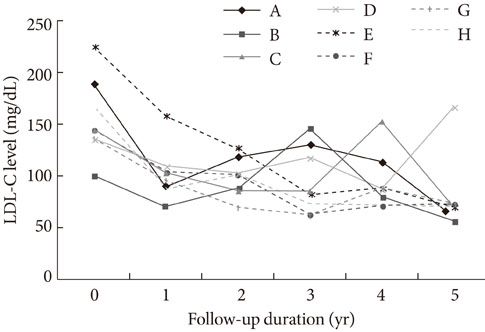
Fig. 2 Low density lipoprotein cholesterol (LDL-C) profiles during the 5 years following initial therapy with atorvastatin 10 mg. Among 28 patients, 8 patients (A-H) used atorvastatin 10 mg as a starting and maintenance dosage without any change in dosage for the entire 5 year period. Of those 8 patients, 7 had final LDL-C levels below 100 mg/dL. Therefore, for this group, the 5-year response rate to an atorvastatin 10 mg fixed dosage was 87.5%.
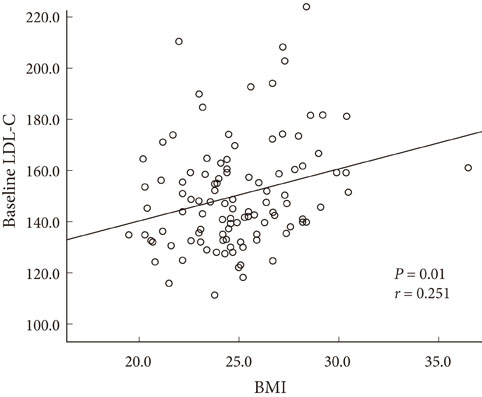
Fig. 3 Correlation between baseline low density lipoprotein cholesterol (LDL-C) levels and body mass index (BMI) (two significant risk factors for short-term non-response).There was significant correlation between these two risk factors. The correlation coefficient was 0.251 (P = 0.01).
Reference
-
1. Stamler J, Vaccaro O, Neaton JD, Wentworth D. Diabetes, other risk factors, and 12-yr cardiovascular mortality for men screened in the Multiple Risk Factor Intervention Trial. Diabetes Care. 1993. 16:434–444.2. Ho JE, Paultre F, Mosca L. Is diabetes mellitus a cardiovascular diseases risk equivalent for fatal stroke in women? Data from the Women's Pooling Project. Stroke. 2003. 34:2812–2816.3. Jeong YJ, Ko SK, Park HS, Yang BM. Meta-analysis and economic evaluation for the effect of statins. J Korean Soc Lipidol Atheroscler. 2004. 14:120–130.4. American Diabetes Association. Position Statement. Management of dyslipidemia in adults with diabetes. Diabetes Care. 2002. 25:Suppl 1. s74–s77.5. American Diabetes Association. Position Statement. Management of dyslipidemia in adults with diabetes. Diabetes Care. 2001. 24:58–61.6. Shepherd J, Cobbe SM, Ford I, Isles CG, Lorimer AR, MacFarlane PW, McKillop JH, Packard CJ. West of Scotland Coronary Prevention Study Group. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. N Engl J Med. 1995. 333:1301–1307.7. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adult Treatment Panel(ATP) III. JAMA. 2001. 285:2486–2497.8. Grundy SM, Cleeman JI, Merz CN, Brewer HB Jr, Clark LT, Hunninghake DB, Pasternak RC, Smith SC Jr, Stone NJ. Coordinating Committee of the National Cholesterol Education Program. Implications of Recent Clinical Trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. Circulation. 2004. 110:227–239.9. National Cholesterol Education Program. Second report of the Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel II). Circulation. 1994. 89:1333–1445.10. Choi DS, Kim DK, Kim DM, Kim SY, Nam MS, Park YS, Shon HS, Ahn CW, Lee KW, Lee KU, Lee MK, Chung CH, Cha BY. 83 investigators. Efficacy evaluation of atorvastatin in Korean hyperlipidemic patients with type 2 diabetes mellitus. J Korean Diabetes Assoc. 2006. 30:292–302.11. Aguilar-Salinas CA, Gomez-Perez FJ, Posadas-Romero C, Vazquez-Chavez C, Meaney E, Gulias-Herrero A, Guillen LE, Alvarado Vega A, Mendoza Perez E, Eduardo Romero-Nava L, Angelica Gomez-Diaz R, Salinas-Orozco S, Moguel R, Novoa G. Efficacy and safety of atorvastatin in hyperlipidemic, type 2 diabetic patients. A 34-week, multicenter, open-label study. Atherosclerosis. 2000. 152:489–496.12. Liao JK. Safety and efficacy of statins in Asians. Am J Cardiol. 2007. 99:410–414.13. Lee E, Ryan S, Birmingham B, Zalikowski J, March R, Ambrose H, Moore R, Lee C, Chen Y, Schneck D. Rosuvastatin pharmacokinetics and pharmacogenetics in white and Asian subjects residing in the same environment. Clin Pharmacol Ther. 2005. 78:330–341.14. Pola P, Kumar R, Reddy AP, Rajagopal G, Harinarayan CV, Suresh V, Suchitra MM, Sachan A. Efficacy of low dose atorvastatin in diabetic dyslipidemia. J Indian Med Assoc. 2009. 107:807–809.15. Cho SW, Lee WR, Lee SY, Namkung J, Do JH. How does atorvastatin 5 mg, simvastatin 10 mg as maintenance therapy meet the therapeutic goal of NCEP ATP III? Korean J Med. 2005. 69:suppl 1. S117.16. Atorvastatin Study Group in Korea. Flexible initial dosing of atorvastatin based upon initial low-density lipoprotein cholesterol levels in type 2 diabetic patients. Korean J Intern Med. 2008. 23:22–29.17. Bae JW, Kim HS, Lee SC, Han KH, Jeon ES. The safety and efficacy of ezetimibe and simvastatin combination therapy in Koreans patients with primary hypercholesterolemia. Korean J Med. 2005. 68:487–497.18. Yi MY, Bae JW, Hwang KK, Kim DW, Cho MC. The effect of dual inhibition of cholesterol in hyperlipidemia patients with acute myocardial infarction. Korean J Med. 2008. 74:59–67.19. Villa J, Prately RE. Ezetimibe/simvastatin or atorvastatin for the treatment of hypercholesterolemia in patients with the metabolic syndrome, the VYMET study. Curr Diab Rep. 2010. 10:173–175.20. Gaede P, Vedel P, Larsen N, Jensen GV, Parving HH, Pedersen O. Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. N Engl J Med. 2003. 348:383–393.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Letter: A Retrospective Study on the Efficacy of a Ten-Milligram Dosage of Atorvastatin for Treatment of Hypercholesterolemia in Type 2 Diabetes Mellitus Patients (Korean Diabetes J 2010;34:359-67)
- Response: A Retrospective Study on the Efficacy of a Ten-Milligram Dosage of Atorvastatin for Treatment of Hypercholesterolemia in Type 2 Diabetes Mellitus Patients (Korean Diabetes J 2010;34:359-67)
- Flexible Initial Dosing of Atorvastatin Based Upon Initial Low-Density Lipoprotein Cholesterol Levels in Type 2 Diabetic Patients
- Dyslipidemia Treatment in Diabetes Mellitus Patients
- Efficacy Evaluation of Atorvastatin in Korean Hyperlipidemic Patients with Type 2 Diabetes Mellitus
