A Rare Manifestation of Hypothyroid Myopathy: Hoffmann's Syndrome
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea. sunhwanae@gmail.com
- 2Department of Neurology, Korea University College of Medicine, Seoul, Korea.
- KMID: 2169677
- DOI: http://doi.org/10.3803/EnM.2015.30.4.626
Abstract
- Hypothyroid myopathy is observed frequently and the resolution of the clinical manifestations of myopathy following thyroid hormone replacement is well known. However, a specific subtype of hypothyroid myopathy, Hoffmann's syndrome, characterized by increased muscular mass (pseudohypertrophy), proximal muscle weakness, muscle stiffness and cramps, is rarely reported. Herein, we describe a 34-year-old male who presented with proximal muscle weakness and non-pitting edema of the lower extremities. He initially visited the neurology department where he was suspected of having polymyositis. Additional laboratory evaluation revealed profound autoimmune hypothyroidism and elevated muscle enzymes including creatine kinase. The patient was started on levothyroxine treatment and, subsequently, clinical symptoms and biochemical parameters resolved with the treatment. The present case highlights that hypothyroidism should be considered in the differential diagnosis of musculoskeletal symptoms even in the absence of overt manifestations of hypothyroidism. To our knowledge, this is the first case reported in Korea.
Keyword
MeSH Terms
Figure
-

Fig. 1 (A) Puffy face and preorbital swelling. (B) Edematous hands and lower legs. (C) Non-pitting edema of the lower extremities and hypertrophy of the calf muscles, with skin changes (dry coarse skin and hyperpigmentation). These photos were taken after obtaining prior consent from the patient.
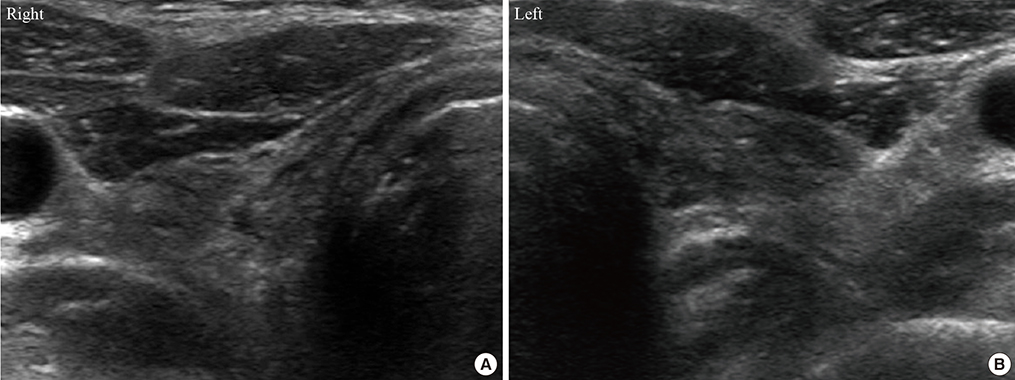
Fig. 2 (A, B) Neck ultrasonography showed atrophied thyroid gland with no definite nodular lesions.
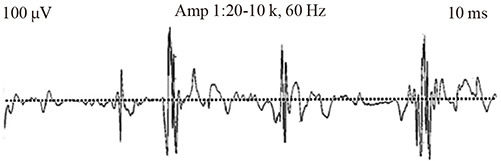
Fig. 3 Electromyography showed mild spontaneous activity and short amplitude with polyphasic myopathic motor unit potential.

Fig. 4 Magnetic resonance imaging of the lower extremities shows symmetric multifocal patchy muscle enhancements with diffuse muscle swelling in both lower legs (superficial posterior compartment). Hypertrophy of the gastrocnemius; affected muscles show hyperintensity on T2-weighted images (arrows).
Reference
-
1. Khaleeli AA, Griffith DG, Edwards RH. The clinical presentation of hypothyroid myopathy and its relationship to abnormalities in structure and function of skeletal muscle. Clin Endocrinol (Oxf). 1983; 19:365–376.2. Madariaga MG. Polymyositis-like syndrome in hypothyroidism: review of cases reported over the past twenty-five years. Thyroid. 2002; 12:331–336.3. Ciompi ML, Zuccotti M, Bazzichi L, Puccetti L. Polymyositis-like syndrome in hypothyroidism: report of two cases. Thyroidology. 1994; 6:33–36.4. Senanayake HM, Dedigama AD, De Alwis RP, Thirumavalavan K. Hoffmann syndrome: a case report. Int Arch Med. 2014; 7:2.5. Qureshi W, Hassan G, Khan GQ, Kadri SM, Kak M, Ahmad M, et al. Hoffmann's syndrome: a case report. Ger Med Sci. 2005; 3:Doc05.6. Vasconcellos LF, Peixoto MC, de Oliveira TN, Penque G, Leite AC. Hoffman's syndrome: pseudohypertrophic myopathy as initial manifestation of hypothyroidism. Case report. Arq Neuropsiquiatr. 2003; 61:851–854.7. Nalini A, Govindaraju C, Kalra P, Kadukar P. Hoffmann's syndrome with unusually long duration: report on clinical, laboratory and muscle imaging findings in two cases. Ann Indian Acad Neurol. 2014; 17:217–221.8. Giampietro O, Clerico A, Buzzigoli G, Del Chicca MG, Boni C, Carpi A. Detection of hypothyroid myopathy by measurement of various serum muscle markers: myoglobin, creatine kinase, lactate dehydrogenase and their isoenzymes. Correlations with thyroid hormone levels (free and total) and clinical usefulness. Horm Res. 1984; 19:232–242.9. Graig FA, Smith JC. Serum creatine phosphokinase activity in altered thyroid states. J Clin Endocrinol Metab. 1965; 25:723–731.10. Mastropasqua M, Spagna G, Baldini V, Tedesco I, Paggi A. Hoffman's syndrome: muscle stiffness, pseudohypertrophy and hypothyroidism. Horm Res. 2003; 59:105–108.11. Finsterer J, Stollberger C, Grossegger C, Kroiss A. Hypothyroid myopathy with unusually high serum creatine kinase values. Horm Res. 1999; 52:205–208.12. Klein I, Mantell P, Parker M, Levey GS. Resolution of abnormal muscle enzyme studies in hypothyroidism. Am J Med Sci. 1980; 279:159–162.13. Tuncel D, Cetinkaya A, Kaya B, Gokce M. Hoffmann's syndrome: a case report. Med Princ Pract. 2008; 17:346–348.14. Khaleeli AA, Gohil K, McPhail G, Round JM, Edwards RH. Muscle morphology and metabolism in hypothyroid myopathy: effects of treatment. J Clin Pathol. 1983; 36:519–526.15. Kaux JF, Castermans C, Delmotte P, Bex M. Hoffmann syndrome presenting to the emergency department. Ann Readapt Med Phys. 2007; 50:310–312.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Acute Rhabdomyolysis as a first Manifestation of Primary Hypothyroidism
- Ataxic Sensory Neuropathy and Polymyositis in Primary Sjogren's Syndrome
- Myasthenia Gravis Occurring Simultaneously With Inflammatory Myopathy in Sjogren's Syndrome
- A case of anterior tibial compartment syndrome induced by bilateral diabetic muscular infarction in hypothyroid state
- A Case of Hypothyroid Myopathy Found in Periodic Health Examination
