Nerves and fasciae in and around the paracolpium or paravaginal tissue: an immunohistochemical study using elderly donated cadavers
- Affiliations
-
- 1Department of Urology, Kobe University Graduate School of Medicine, Kobe, Japan. hinata@med.kobe-u.ac.jp
- 2Department of Urology, Hiroshima University School of Medicine, Hiroshima, Japan.
- 3Division of Gynecology and Obstetrics, Ishikawa Prefectural Central Hospital, Kanazawa, Japan.
- 4Department of Gynecology and Obstetrics, Fukui University School of Medicine, Fukui, Japan.
- 5Division of Internal Medicine, Iwamizawa Kojin-kai Hospital, Iwamizawa, Japan.
- 6Department of Anatomy, Sapporo Medical University School of Medicine, Sapporo, Japan.
- KMID: 2168856
- DOI: http://doi.org/10.5115/acb.2014.47.1.44
Abstract
- The paracolpium or paravaginal tissue is surrounded by the vaginal wall, the pubocervical fascia and the rectovaginal septum (Denonvilliers' fascia). To clarify the configuration of nerves and fasciae in and around the paracolpium, we examined histological sections of 10 elderly cadavers. The paracolpium contained the distal part of the pelvic autonomic nerve plexus and its branches: the cavernous nerve, the nerves to the urethra and the nerves to the internal anal sphincter (NIAS). The NIAS ran postero-inferiorly along the superior fascia of the levator ani muscle to reach the longitudinal muscle layer of the rectum. In two nulliparous and one multiparous women, the pubocervical fascia and the rectovaginal septum were distinct and connected with the superior fascia of the levator at the tendinous arch of the pelvic fasciae. In these three cadavers, the pelvic plexus and its distal branches were distributed almost evenly in the paracolpium and sandwiched by the pubocervical and Denonvilliers' fasciae. By contrast, in five multiparous women, these nerves were divided into the anterosuperior group (bladder detrusor nerves) and the postero-inferior group (NIAS, cavernous and urethral nerves) by the well-developed venous plexus in combination with the fragmented or unclear fasciae. Although the small number of specimens was a major limitation of this study, we hypothesized that, in combination with destruction of the basic fascial architecture due to vaginal delivery and aging, the pelvic plexus is likely to change from a sheet-like configuration to several bundles.
Keyword
MeSH Terms
Figure
-
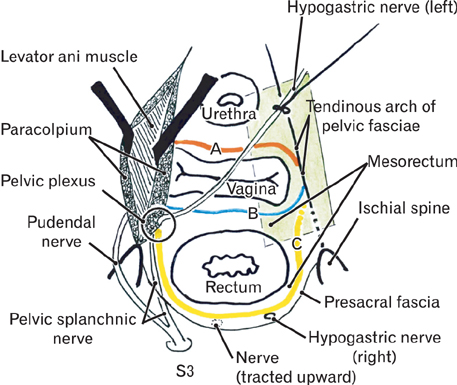
Fig. 1 Schematic representation of the pelvic fasciae along and around the vagina. The right-hand side of the figure displays fascial connections with the superior fascia of the levetor anti-muscle at the tendinous arch of the pelvic fasciae: the pubocervical fascia (red line marked A) joins not only the rectovaginal septum (Denonvilliers' fascia; blue line marked B) but also, possibly, a fascia around the mesorectum (yellow line marked C). The mesorectum (a surgical term) does not correspond to the true mesentery but a loose mass of fatty tissue surrounding the lower rectum. The green colored square indicates the plane used for most of photographic demonstrations in the present study: it includes the 3 visceral systems in the pelvis (the urologic system, the reproductive system, and the alimentary canal) as well as the tendinous arch of the pelvic fasciae. The left hand-side of the figure shows a partial dissection of the paravaginal tissue or paracolpium. The paracolpium in the present study is likely to include at least some parts of the pelvic autonomic nerve plexus (pelvic plexus). The bilateral hypogastric nerve (left) is also dissected to show its arrival at the pelvic plexus area. The pelvic splanchnic nerve runs along the anteromedial side of the ischial spine, while the pudendal nerve runs along the posterolateral side. S3, third sacral nerve root.

Fig. 2 Histology of a specimen from a 79-year-old nulliparous woman. Tilted frontal planes. Panels (A-C) display macroscopic slices before histologic preparation. Panel (A) represents the most posterosuperior side of the 3 panels, while panel (C) represents the most antero-inferior side. The posterior end of the urinary bladder (B) is seen in panel (C). Stars indicate the superior fascia of the levator ani muscle. Intervals between panels are about 15 mm. Panels (D-F) exhibit hematoxylin and eosin sections at the same lower magnification corresponding to the central parts of panels (A-C), respectively. Scale bar in panel (D)=10 mm (D-F). The rectovaginal septum (Denonvilliers' fas cia; RVS) and the pubocervical fascia (PCF) are seen connecting with the superior fascia (stars) of the levator ani muscle (LA). Panels (G-I; same magnification) correspond to the squares in panels (E) and (F). Scale bar in panel (H, I)=0.1 mm (G-I). Panels (G) and (H) (immunohistochemistry for smooth muscle actin) show smooth muscles in the PCF (G) and recto vaginal septum (H). Panel (I) (elastica-Masson staining) shows smooth muscles and elastic fibers (black lines) in the superior fascia of the levator. ATFP, arcus tendineus fasciae pelvis; EAS, external anal sphincter; IF, ischorectal fossa; OI, obturator internus muscle; R, rectum; SRA&V, branches and tributaries of the su perior rectal artery and vein; UR, ure ter; UT, uterus; VAG, vagina.
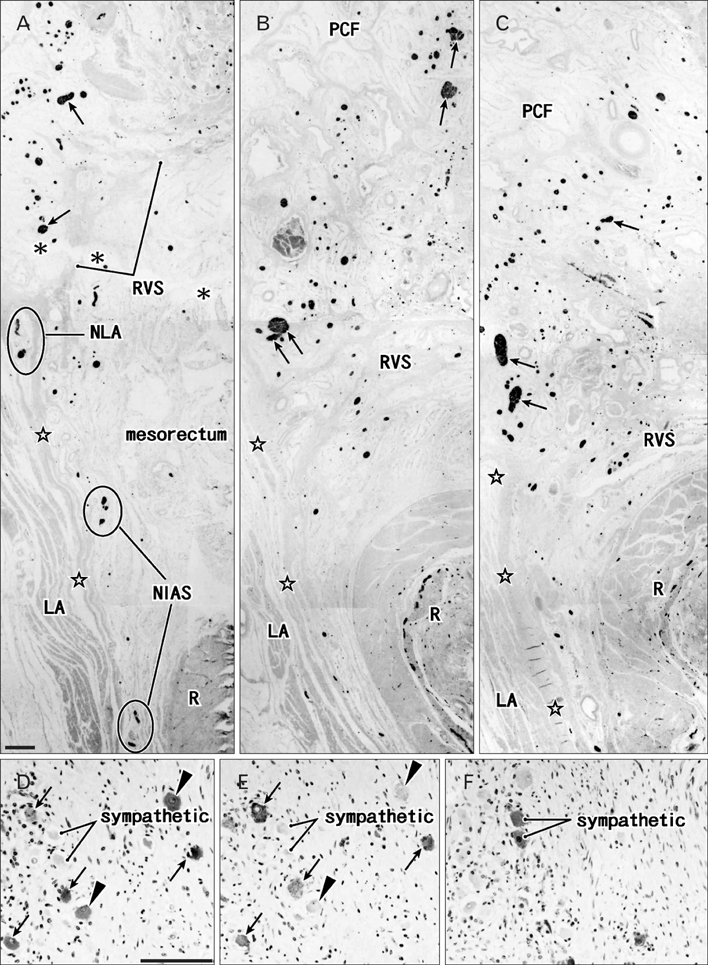
Fig. 3 S100 immunohistochemistry of nerves in the paracolpium of the specimen shown in Fig. 2. Panels (A), (B), and (C) (same magnification) cor respond to the central parts of Fig. 2D, E and F, respectively, and display nerves in the paracolpium. Scale bar in panel (A)=1 mm (A-C). S100-positive nerves are distributed almost evenly in the lateral part of the paracolpium. Nerves with arrows contain ganglion cell clusters. Asterisks in panel (A) indicate an artifactual cleft created by the histo logical procedure. Panels (D), (E) and (F) (same magnification) show immunohistochemistry of neuronal nitric oxide synthase (nNOS), vasoactive intestinal peptide (VIP), and tyrosine hydroxylase (TH) in adjacent sections of a ganglion cell cluster in panel (C), respectively. Scale bar in panel (D)=0.1 mm (D-F). Most of the nNOS-positive cells (arrows in panels D and E; parasympathetic) appear to express VIP (i.e., double positive) with a few exceptions (arrowheads). The cluster also con tains TH-positive sympathetic nerve cells (F). Nerves to the internal anal sphincter (NIAS) (or nerves to the levator ani) candidate nerves extending to the internal anal sphincter (those to the levator ani muscle [LA]). PCF, pubocervical fascia; R, rectum; RVS, recto vaginal septum.
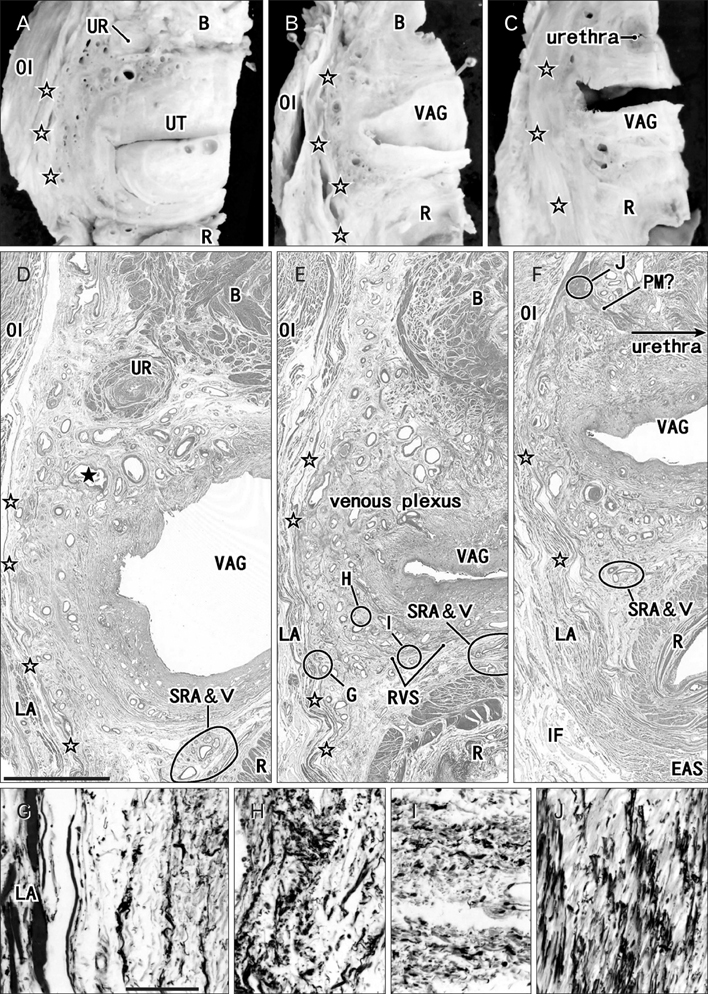
Fig. 4 Histology of a specimen from a 73-year-old multiparous woman. Tilted frontal planes. Panels (A-C) display macroscopic slices before histologic preparation. Panel (A) represents the most posterosuperior side of the 3 panels, while panel (C) represents the most antero-inferior side. The inferior end of the urinary bladder (B) is seen in panel (C). Open stars indicate the superior fascia of the levator ani muscle. Intervals between panels are about 15 mm. Panels (D-F) exhibit hematoxylin and eosin sections at the same lower magnification corresponding to the central parts of panels (A-C), respectively. Scale bar in panel (D)=10 mm (D-F). Parts of the rectovaginal septum (Denonvilliers' fascia; RVS) are seen, but the pubocervical fascia (PCF) is fragmented in panels (A) and (B). Panels (G-J) (same magnification) are higher-magnification views (elastica-Masson staining) of the circles marked G, H, I, and J in panels (E) and (F), respectively. Scale bar in panel (G)=0.1 mm (G-J). Elastic fibers are stained black. A candidate for the perineal membrane (PM) in panel (J) contains regularly arrayed elastic fibers. Black star in panel (D) corresponds to that in Fig. 5A. EAS, external anal sphincter; IF, ischorectal fossa; LA, levator ani muscle; OI, obturator internus muscle; R, rectum; SRA&V, branches and tributaries of the superior rectal artery and vein; UR, ureter; UT, uterus; VAG, vagina.

Fig. 5 S100 immunohistochemistry of nerves in the paracolpium of the specimen shown in Fig. 4. Panels (A), (B), and (C) (same magnification) correspond to the central parts of Fig. 4D, E and F, respectively, and display nerves in the paracolpium. Scale bar in panel (A)=1 mm (A-C). Black star in panel (A) corresponds to that in Fig. 4D. In panel (C), the venous plexus divides the nerves into two groups: one of the groups is located close to the superior rectal artery and vein (SRA&V). Nerves with an arrow contain ganglion cell clusters. Panels (D-F) (same magnification) show immunohistochemistry of adjacent sections of a nerve in panel (B). Scale bar in panel (D)=0.1 mm (D-F). The neuronal nitric oxide synthase (nNOS)-positive parasym pathetic nerve fibers (D) as well as tyrosine hydroxylase (TH)-positive sympathetic nerve fibers (F) are evenly distributed in the nerve, while vasoactive intestinal peptide (VIP)-positive parasympathetic nerve fibers tend to be restricted to the right-hand side of the nerve (E). Nerves to the internal anal sphincter (NIAS) (or NLA) candidate nerves extending to the internal anal sphincter (those to the levator ani muscle). Other abbreviations are the same as in Fig. 2. LA, levator ani muscle; VAG, vagina.
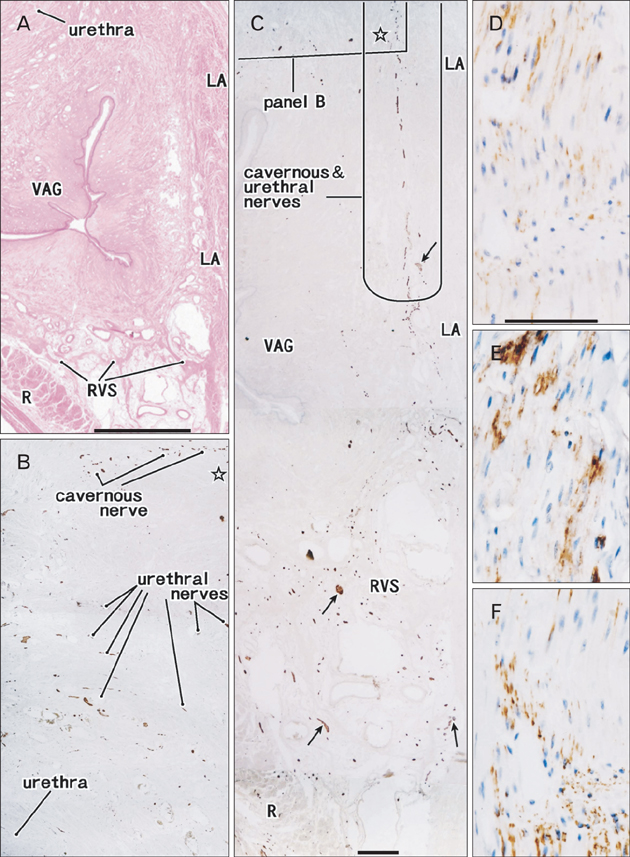
Fig. 6 Candidates for the cavernous and urethral nerves in an 88-year-old multiparous woman. Tilted frontal planes. Panel (A) (hamatoxylin and eosin staining) displays a low-magnification view including the paracolpium. Scale bar in panel (A)=10 mm. Panels (B) and (C) show S100 immunohistochemistry: panel (B) cor responds to the square in the up per margin of panel (C), while panel (C) shows areas along the levator ani muscle (LA) in panel (A). Scale bar in panel (C)=1 mm (B, C). Open star in panels (B) and (C) indicates a same site for comparison. In panel (C), candidates for the cavernous and urethral nerves run anteriorly along the lateral side of the vagina (VAG). Nerves with an arrow contain ganglion cell clusters (B). Panels (D-F) (same magnification) show immunohistochemistry in sections adjacent to the cavernous nerve candidate in panel (C). Scale bar in panel (D)=0.1 mm (D-F). Most of the parasympathetic nerve fibers appear to express both nNOS (D) and VIP (E), i.e., double positive. The nerve also contains tyrosine hydroxylase-positive sympathetic nerve fibers (F). R, rectum; RVS, rectovaginal septum.
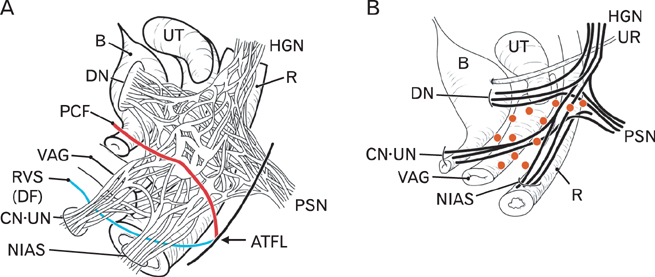
Fig. 7 Hypothetical change in the morphology of the pelvic plexus from a sheet to several bundles in combination with destruction of the covering fascias due to vaginal delivery and aging. Panel (A) displays the basic configuration without destruction of the pelvic fasciae. The pelvic plexus takes a sheet-like configuration comprising a complex of almost evenly distributed nerves. In these branches, the bladder detrusor nerves (DN) were greatest in number, while the cavernous nerve (CN), the nerves to the urethral sphincters (urethral nerve or UN) and the nerves to the internal anal sphincter (NIAS) were relatively fewer. The distal parts of the pelvic plexus and its branches were located in a space between the pubocervical fascia (PCF) and the rectovaginal septum (RVS=Denonvilliers' fascia or DF). Panel (B) shows the change in shape of the plexus in combination with destruction of the definite fasciae along the vagina due to the secondarily developed venous plexus (orange dots). The distal branches are not evenly distributed but form several bundles. ATFL, arcus tendineus fasciae pelvis; B, urinary bladder; HGN, hypogastric nerve; PSN, pelvic splanchnic nerve; R, rectum; UR, ureter; UT, uterus; VAG, vagina.
Reference
-
1. DeLancey JO. Anatomic aspects of vaginal eversion after hysterectomy. Am J Obstet Gynecol. 1992; 166(6 Pt 1):1717–1724.2. Mostwin JL. Current concepts of female pelvic anatomy and physiology. Urol Clin North Am. 1991; 18:175–195.3. Mauroy B, Goullet E, Stefaniak X, Bonnal JL, Amara N. Tendinous arch of the pelvic fascia: application to the technique of paravaginal colposuspension. Surg Radiol Anat. 2000; 22:73–79.4. Pit MJ, De Ruiter MC, Lycklama AN, Marani E, Zwartendijk J. Anatomy of the arcus tendineus fasciae pelvis in females. Clin Anat. 2003; 16:131–137.5. Albright TS, Gehrich AP, Davis GD, Sabi FL, Buller JL. Arcus tendineus fascia pelvis: a further understanding. Am J Obstet Gynecol. 2005; 193(3 Pt 1):677–681.6. Zhai LD, Liu J, Li YS, Yuan W, He L. Denonvilliers' fascia in women and its relationship with the fascia propria of the rectum examined by successive slices of celloidin-embedded pelvic viscera. Dis Colon Rectum. 2009; 52:1564–1571.7. Zhang C, Ding ZH, Li GX, Yu J, Wang YN, Hu YF. Perirectal fascia and spaces: annular distribution pattern around the mesorectum. Dis Colon Rectum. 2010; 53:1315–1322.8. Donker PJ. A study of the myelinated fibres in the branches of the pelvic plexus. Neurourol Urodyn. 1986; 5:185–202.9. Ball TP Jr, Teichman JM, Sharkey FE, Rogenes VJ, Adrian EK Jr. Terminal nerve distribution to the urethra and bladder neck: considerations in the management of stress urinary incontinence. J Urol. 1997; 158(3 Pt 1):827–829.10. Kato M, Niikura H, Yaegashi N, Murakami G, Tatsumi H, Matsubara A. Histotopography of the female cavernous nerve: a study using donated fetuses and adult cadavers. Int Urogynecol J Pelvic Floor Dysfunct. 2008; 19:1687–1695.11. Hirata E, Koyama M, Murakami G, Ohtsuka A, Abe S, Ide Y, Fujiwara H, Kudo Y. Comparative histological study of levels 1-3 supportive tissues using pelvic floor semiserial sections from elderly nulliparous and multiparous women. J Obstet Gynaecol Res. 2011; 37:13–23.12. Yucel S, De Souza A Jr, Baskin LS. Neuroanatomy of the human female lower urogenital tract. J Urol. 2004; 172:191–195.13. Alsaid B, Moszkowicz D, Peschaud F, Bessede T, Zaitouna M, Karam I, Droupy S, Benoit G. Autonomic-somatic communications in the human pelvis: computer-assisted anatomic dissection in male and female fetuses. J Anat. 2011; 219:565–573.14. Hieda K, Cho KH, Arakawa T, Fujimiya M, Murakami G, Matsubara A. Nerves in the intersphincteric space of the human anal canal with special reference to their continuation to the enteric nerve plexus of the rectum. Clin Anat. 2013; 03. 20. [Epub]. http://dx.doi.org/10.1002/ca.22227.15. Hoyle CH, Stones RW, Robson T, Whitley K, Burnstock G. Innervation of vasculature and microvasculature of the human vagina by NOS and neuropeptide-containing nerves. J Anat. 1996; 188(Pt 3):633–644.16. Maas CP, DeRuiter MC, Kenter GG, Trimbos JB. The inferior hypogastric plexus in gynecologic surgery. J Gynecol Tech. 1999; 5:55–62.17. Baader B, Herrmann M. Topography of the pelvic autonomic nervous system and its potential impact on surgical intervention in the pelvis. Clin Anat. 2003; 16:119–130.18. Ercoli A, Delmas V, Fanfani F, Gadonneix P, Ceccaroni M, Fagotti A, Mancuso S, Scambia G. Terminologia Anatomica versus unofficial descriptions and nomenclature of the fasciae and ligaments of the female pelvis: a dissection-based comparative study. Am J Obstet Gynecol. 2005; 193:1565–1573.19. Yabuki Y, Sasaki H, Hatakeyama N, Murakami G. Discrepancies between classic anatomy and modern gynecologic surgery on pelvic connective tissue structure: harmonization of those concepts by collaborative cadaver dissection. Am J Obstet Gynecol. 2005; 193:7–15.20. Hollabaugh RS, Steiner MS, Dmochowski RR. Neuroanatomy of the female continence complex: clinical implications. Urology. 2001; 57:382–388.21. Tamakawa M, Murakami G, Takashima K, Kato T, Hareyama M. Fascial structures and autonomic nerves in the female pelvis: a study using macroscopic slices and their corresponding histology. Anat Sci Int. 2003; 78:228–242.22. Motohashi O, Suzuki M, Shida N, Umezawa K, Ohtoh T, Sakurai Y, Yoshimoto T. Subarachnoid haemorrhage induced proliferation of leptomeningeal cells and deposition of extracellular matrices in the arachnoid granulations and subarachnoid space. Immunhistochemical study. Acta Neurochir (Wien). 1995; 136:88–91.23. Hayashi T, Kumasaka T, Mitani K, Yao T, Suda K, Seyama K. Loss of heterozygosity on tuberous sclerosis complex genes in multifocal micronodular pneumocyte hyperplasia. Mod Pathol. 2010; 23:1251–1260.24. Kato M, Matsubara A, Murakami G, Abe S, Ide Y, Sato I, Usui T. Female perineal membrane: a study using pelvic floor semiserial sections from elderly nulliparous and multiparous women. Int Urogynecol J Pelvic Floor Dysfunct. 2008; 19:1663–1670.25. Niikura H, Jin ZW, Cho BH, Murakami G, Yaegashi N, Lee JK, Lee NH, Li CA. Human fetal anatomy of the coccygeal attachments of the levator ani muscle. Clin Anat. 2010; 23:566–574.26. Hinata N, Murakami G, Abe S, Honda M, Isoyama T, Sejima T, Takenaka A. Detailed histological investigation of the female urethra: application to radical cystectomy. J Urol. 2012; 187:451–456.27. Takenaka A, Soga H, Murakami G, Niikura H, Tatsumi H, Yaegashi N, Tanaka K, Fujisawa M. Understanding anatomy of "hilus" of detrusor nerves to avoid bladder dysfunction after pelvic surgery: demonstration using fetal and adult cadavers . Urology. 2009; 73:251–257.28. Leffler KS, Thompson JR, Cundiff GW, Buller JL, Burrows LJ, Schön Ybarra MA. Attachment of the rectovaginal septum to the pelvic sidewall. Am J Obstet Gynecol. 2001; 185:41–43.29. Nagata I, Murakami G, Suzuki D, Furuya K, Koyama M, Ohtsuka A. Histological features of the rectovaginal septum in elderly women and a proposal for posterior vaginal defect repair. Int Urogynecol J Pelvic Floor Dysfunct. 2007; 18:863–868.30. Hirata E, Fujiwara H, Hayashi S, Ohtsuka A, Abe S, Murakami G, Kudo Y. Intergender differences in histological architecture of the fascia pelvis parietalis: a cadaveric study. Clin Anat. 2011; 24:469–477.31. Takeyama M, Koyama M, Murakami G, Nagata I, Tomoe H, Furuya K. Nerve preservation in tension-free vaginal mesh procedures for pelvic organ prolapse: a cadaveric study using fresh and fixed cadavers. Int Urogynecol J Pelvic Floor Dysfunct. 2008; 19:559–566.32. Arakawa T, Murakami G, Nakajima F, Matsubara A, Ohtsuka A, Goto T, Teramoto T. Morphologies of the interfaces between the levator ani muscle and pelvic viscera, with special reference to muscle insertion into the anorectum in elderly Japanese. Anat Sci Int. 2004; 79:72–81.33. Kinugasa Y, Murakami G, Suzuki D, Sugihara K. Histological identification of fascial structures posterolateral to the rectum. Br J Surg. 2007; 94:620–626.34. Sato K, Sato T. The vascular and neuronal composition of the lateral ligament of the rectum and the rectosacral fascia. Surg Radiol Anat. 1991; 13:17–22.35. Lin M, Chen W, Huang L, Ni J, Yin L. The anatomy of lateral ligament of the rectum and its role in total mesorectal excision. World J Surg. 2010; 34:594–598.36. Açar HI, Kuzu MA. Important points for protection of the autonomic nerves during total mesorectal excision. Dis Colon Rectum. 2012; 55:907–912.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Topohistology of sympathetic and parasympathetic nerve fibers in branches of the pelvic plexus: an immunohistochemical study using donated elderly cadavers
- Anatomical and Radiological Study of the Vascular Distribution and Skin Territory for the Tensor Fasciae Latae Free Flap
- Laparoscopic Paravaginal repair for the Treatment of Symptomatic Cystocele
- Composite nerve fibers in the hypogastric and pelvic splanchnic nerves: an immunohistochemical study using elderly cadavers
- A Case Report of a Huge Epidermal Inclusion Cyst in the Paravaginal Space
