Successful Treatment by Chemotherapy of Pineal Parenchymal Tumor with Intermediate Differentiation: A Case Report
- Affiliations
-
- 1Department of Internal Medicine, Pusan National University Hospital, Pusan University College of Medicine, Busan, Korea. chyj@pnuh.co.kr
Abstract
- A 37-year-old male presented with a mass measuring 2.5 cm in size in the midbrain and obstructive hydrocephalus, which had manifested as a headache and dizziness. Magnetic resonance (MR) imaging of the brain showed intermediate enhancement on T1-weighted MR imaging and a high intensity of enhancement on T2-weighted MR. Neurosurgeons performed an occipital craniotomy with partial removal of the tumor and the postoperative diagnosis was a pineal parenchymal tumor with intermediate differentiation. He had undergone irradiation with 54 Gy of radiation on 27 fractions for removal of the remaining tumor approximately one month after surgery. However, in follow-up imaging performed four months after radiotherapy, a remnant mass in the superoposterior aspect of the midbrain was found to have extended to the hypothalamus and the third ventricle. He was treated with six cycles of procarbazine, lomustine, vincristine chemotherapy. At five months since the completion of chemotherapy, the brain MR imaging showed no evidence of any remaining tumor and he no longer displayed any of his initial symptoms.
Keyword
MeSH Terms
Figure
-
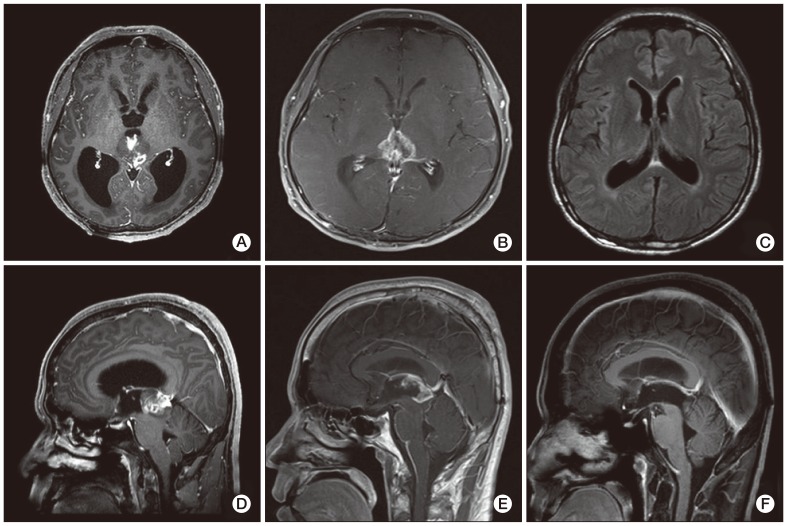
Fig. 1 Magnetic resonance imaging. (A, D) Pre-operative T1-weighed sagital and axial images showed a well enhanced pineal mass that had invaded the midbrain. It also showed an obstructive hydrocephalus. (B, E) The remnant mass had extended into both sides of the hypothalamus and third ventricle after surgical removal and radiotherapy. In addition, leptomeningeal enhancement was observed in the infratentorial fossa, indicating cerebrospinal fluid seeding. (C, F) No evidence of any remnant mass after chemotherapy.

Fig. 2 Pathology. (A) Histology. The majority of the tumor tissue exhibited small hyperchromatic cells with moderately increased cellularity and a high nuclear to cytoplasmic ratio. The tumor cells showed mild atypical mitosis, however, rare mitotic activity was observed. Giant cells were also observed (H&E staining, ×1,000). (B) Immunohistochemistry. Tumor cells exhibited focal staining for synaptophysin (×40).
Reference
-
1. Jakacki RI, Zeltzer PM, Boyett JM, Albright AL, Allen JC, Geyer JR, et al. Survival and prognostic factors following radiation and/or chemotherapy for primitive neuroectodermal tumors of the pineal region in infants and children: a report of the Childrens Cancer Group. J Clin Oncol. 1995; 13:1377–1383. PMID: 7751882.
Article2. Jouvet A, Saint-Pierre G, Fauchon F, Privat K, Bouffet E, Ruchoux MM, et al. Pineal parenchymal tumors: a correlation of histological features with prognosis in 66 cases. Brain Pathol. 2000; 10:49–46. PMID: 10668895.
Article3. Fauchon F, Jouvet A, Paquis P, Saint-Pierre G, Mottolese C, Ben Hassel M, et al. Parenchymal pineal tumors: a clinicopathological study of 76 cases. Int J Radiat Oncol Biol Phys. 2000; 46:959–968. PMID: 10705018.
Article4. Kim BS, Kim DK, Park SH. Pineal parenchymal tumor of intermediate differentiation showing malignant progression at relapse. Neuropathology. 2009; 29:602–608. PMID: 19170892.
Article5. Kurisaka M, Arisawa M, Mori T, Sakamoto T, Seike M, Mori K, et al. Combination chemotherapy (cisplatin, vinblastin) and low-dose irradiation in the treatment of pineal parenchymal cell tumors. Childs Nerv Syst. 1998; 14:564–569. PMID: 9840380.
Article6. Report of Brain Tumor Registry of Japan (1969-1993). Neurol Med Chir (Tokyo). 2000; 40(Suppl):1–106.7. Schild SE, Scheithauer BW, Schomberg PJ, Hook CC, Kelly PJ, Frick L, et al. Pineal parenchymal tumors: clinical, pathologic, and therapeutic aspects. Cancer. 1993; 72:870–880. PMID: 8334641.
Article8. Duffner PK, Cohen ME, Sanford RA, Horowitz ME, Krischer JP, Burger PC, et al. Pediatric Oncology Group. Lack of efficacy of postoperative chemotherapy and delayed radiation in very young children with pineoblastoma. Med Pediatr Oncol. 1995; 25:38–44. PMID: 7753001.
Article9. Gururangan S, McLaughlin C, Quinn J, Rich J, Reardon D, Halperin EC, et al. High-dose chemotherapy with autologous stem-cell rescue in children and adults with newly diagnosed pineoblastomas. J Clin Oncol. 2003; 21:2187–2191. PMID: 12775745.
Article10. Ghim TT, Davis P, Seo JJ, Crocker I, O'Brien M, Krawiecki N. Response to neoadjuvant chemotherapy in children with pineoblastoma. Cancer. 1993; 72:1795–1800. PMID: 8348511.
Article11. Kurisaka M, Arisawa M, Moriki A, Mori K. Successful combination chemotherapy (cisplatin, vinblastine, and bleomycin) with small-dose irradiation in the treatment of pineoblastoma metastasized into spinal cord: case report. Surg Neurol. 1993; 39:152–157. PMID: 7688912.
Article12. Anan M, Ishii K, Nakamura T, Yamashita M, Katayama S, Sainoo M, et al. Postoperative adjuvant treatment for pineal parenchymal tumour of intermediate differentiation. J Clin Neurosci. 2006; 13:965–968. PMID: 16904896.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pineal Parenchymal Tumor of Intermediate Differentiation with Gangliocytic Differentiation: A Case Report
- Pineal Anlage Tumor: A case report
- Upfront Stereotactic Radiosurgery for Pineal Parenchymal Tumors in Adults
- Pineoblastoma with Neuronal Differentiation: A case report
- Survival and Malignant Transformation of Pineal Parenchymal Tumors: A 30-Year Retrospective Analysis in a Single-Institution
