Ratio of Leukotriene E4 to Exhaled Nitric Oxide and the Therapeutic Response in Children With Exercise-Induced Bronchoconstriction
- Affiliations
-
- 1Department of Pediatrics, Kangdong Sacred Heart Hospital, Hallym University School of Medicine, Seoul, Korea.
- 2Department of Biochemistry and Molecular Biology, Hanyang University School of Medicine, Seoul, Korea.
- 3Department of Pediatrics, Hanyang University School of Medicine, Seoul, Korea. hablee@hanyang.ac.kr
- KMID: 2167003
- DOI: http://doi.org/10.4168/aair.2013.5.1.26
Abstract
- PURPOSE
This study assessed the association between the ratio of leukotriene E4 (LTE4) to fractional exhaled nitric oxide (FENO) in the response of children with exercise-induced bronchoconstriction (EIB) enrolled in a therapeutic trial with montelukast or inhaled corticosteroid (fluticasone propionate [FP]).
METHODS
Children aged 6 to 18 years with EIB were randomized in a 4-week, placebo-controlled, double-blinded trial with montelukast or FP. Before and after treatment, treadmill exercise challenges were performed. The LTE4 levels in the induced sputum and urine and the FENO levels were measured in subjects before and 30 minutes after the exercise challenges. The same tests were conducted after treatment.
RESULTS
A total of 24 patients completed the study: 12 in the montelukast group and 12 in FP group. Both study groups displayed a similar postexercise maximum decrease in forced expiratory volume in one second (FEV1) before treatment as well as after treatment. However, there were significant differences in the magnitude of change between the two (Delta; -18.38+/-14.53% vs. -4.67+/-8.12% for the montelukast and FP groups, respectively; P=0.021). The Delta logarithmic sputum baseline and postexercise LTE4/FENO ratio were significantly lower in the montelukast group than in the FP group (baseline; -0.09+/-0.21 vs. -0.024+/-0.03, P=0.045; postexercise, -0.61+/-0.33 vs. -0.11+/-0.28, P=0.023).
CONCLUSIONS
These data indicate that the efficacy of montelukast for preventing a maximum decrease in FEV1 after exercise is significantly higher than that of FP, and the high LTE4/FENO ratio is associated with a greater response to montelukast than to FP for EIB therapy. These results suggest that LTE4 may play an important role in EIB.
Keyword
MeSH Terms
Figure
-

Fig. 1 Sputum and urinary LTE4/FENO, baseline and postexercise, before and after treatment in the two study groups of asthma. There were significant differences in the sputum LTE4/FENO ratio at baseline and postexercise after treatment compared to those before treatment in the montelukast group (baseline, 25.66±23.47 vs. 8.42±8.01, P=0.008; postexercise, 45.72±52.94 vs. 16.63±15.26, P=0.001) (A) and in the FP group (baseline, 25.24±17.58 vs. 20.41±17.54, P=0.048; postexercise, 51.10±47.91 vs. 45.79±39.86, P=0.044) (B). There were significant differences in the urine LTE4/FENO ratio at baseline and postexercise between treatments in the montelukast group (baseline, 2.36±2.37 vs. 0.88±0.38, P=0.012; postexercise, 2.53±1.64 vs. 1.04±0.68) (C) and in the FP group (baseline, 2.23±2.01 vs. 1.60±1.48, P=0.038; postexercise, 2.28±1.75 vs. 1.71±1.39, P=0.043) (D).
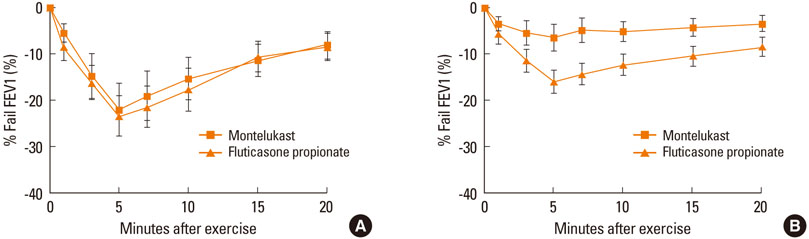
Fig. 2 Mean±SE changes in percent decrease FEV1 after exercise challenge before treatment (A) and after 4 weeks of asthma treatment (B) with montelukast (n=12) or FP (n=12). No significant differences were observed in the postexercise maximum decrease in FEV1 and area under the FEV1 curve over the first 20 min after exercise (AUC20) before treatment between two groups (A). Postexercise maximum decrease in FEV1 and AUC20 in the montelukast group were significantly lower compared to those of the FP group after treatment (8.83±7.74% vs. 16.54±7.71%, P=0.024; 232.1±187.9 vs. 374.9±145.0, P=0.035) (B).

Fig. 3 Difference between two measurements after and before treatment for the montelukast and FP groups. There were significant differences in the Δpostexercise maximum decrease in FEV1 between the montelukast group and the FP group (-18.38±14.53% vs. -4.67±8.12%, P=0.021) (A). There were significant differences in the ΔAUC20 between the montelukast group and the FP group (-21.23±17.53 vs. -3.72±3.81, P=0.028) (B). The Δ logarithmic sputum baseline and postexercise LTE4/FENO ratio were significantly lower in the montelukast group compared to the FP group [baseline, -0.09±0.21 vs. -0.024±0.03, P=0.045 (C); postexercise, -0.61±0.33 vs. -0.11±0.28, P=0.023 (D)]. The Δ logarithmic urinary baseline and postexercise LTE4/FENO ratio were significantly lower in the montelukast group compared to the FP group [baseline, -0.60±0.21 vs. -0.084±0.14, P=0.046 (E); postexercise, -0.30±0.25 vs. -0.16±0.16, P=0.038 (F)]. Δ, measurementafter treatment - measurementbefore treatment; FP, fluticasone propionate. *P<0.05 Montelukast vs. FP, analyzed by a Mann-Whitney test.
Reference
-
1. Cabral AL, Conceição GM, Fonseca-Guedes CH, Martins MA. Exercise-induced bronchospasm in children: effects of asthma severity. Am J Respir Crit Care Med. 1999. 159:1819–1823.2. Joos GF, O'Connor B, Anderson SD, Chung F, Cockcroft DW, Dahlén B, DiMaria G, Foresi A, Hargreave FE, Holgate ST, Inman M, Lötvall J, Magnussen H, Polosa R, Postma DS, Riedler J. ERS Task Force. Indirect airway challenges. Eur Respir J. 2003. 21:1050–1068.3. Jones A. Screening for asthma in children. Br J Gen Pract. 1994. 44:179–183.4. Holgate ST, Lemanske RF Jr, O'Byrne PM, Kakumanu S, Busse WW. Adkinson NF, Yunginger JW, Busse WW, Bochner BS, Holgate ST, Simon FE, editors. Asthma pathogenesis. Middleton's allergy: principles and practice. 2009. 7th ed. Philadelphia: Mosby;893.5. O'Sullivan S, Roquet A, Dahlén B, Larsen F, Eklund A, Kumlin M, O'Byrne PM, Dahlén SE. Evidence for mast cell activation during exercise-induced bronchoconstriction. Eur Respir J. 1998. 12:345–350.6. Gauvreau GM, Ronnen GM, Watson RM, O'Byrne PM. Exercise-induced bronchoconstriction does not cause eosinophilic airway inflammation or airway hyperresponsiveness in subjects with asthma. Am J Respir Crit Care Med. 2000. 162:1302–1307.7. Carroll NG, Mutavdzic S, James AL. Distribution and degranulation of airway mast cells in normal and asthmatic subjects. Eur Respir J. 2002. 19:879–885.8. Karjalainen EM, Laitinen A, Sue-Chu M, Altraja A, Bjermer L, Laitinen LA. Evidence of airway inflammation and remodeling in ski athletes with and without bronchial hyperresponsiveness to methacholine. Am J Respir Crit Care Med. 2000. 161:2086–2091.9. Hallstrand TS, Moody MW, Aitken ML, Henderson WR Jr. Airway immunopathology of asthma with exercise-induced bronchoconstriction. J Allergy Clin Immunol. 2005. 116:586–593.10. Hallstrand TS, Moody MW, Wurfel MM, Schwartz LB, Henderson WR Jr, Aitken ML. Inflammatory basis of exercise-induced bronchoconstriction. Am J Respir Crit Care Med. 2005. 172:679–686.11. Reiss TF, Hill JB, Harman E, Zhang J, Tanaka WK, Bronsky E, Guerreiro D, Hendeles L. Increased urinary excretion of LTE4 after exercise and attenuation of exercise-induced bronchospasm by montelukast, a cysteinyl leukotriene receptor antagonist. Thorax. 1997. 52:1030–1035.12. Leff JA, Busse WW, Pearlman D, Bronsky EA, Kemp J, Hendeles L, Dockhorn R, Kundu S, Zhang J, Seidenberg BC, Reiss TF. Montelukast, a leukotriene-receptor antagonist, for the treatment of mild asthma and exercise-induced bronchoconstriction. N Engl J Med. 1998. 339:147–152.13. Waalkens HJ, van Essen-Zandvliet EE, Gerritsen J, Duiverman EJ, Kerrebijn KF, Knol K. Dutch CNSLD Study Group. The effect of an inhaled corticosteroid (budesonide) on exercise-induced asthma in children. Eur Respir J. 1993. 6:652–656.14. Freezer NJ, Croasdell H, Doull IJ, Holgate ST. Effect of regular inhaled beclomethasone on exercise and methacholine airway responses in school children with recurrent wheeze. Eur Respir J. 1995. 8:1488–1493.15. de Benedictis FM, del Giudice MM, Forenza N, Decimo F, de Benedictis D, Capristo A. Lack of tolerance to the protective effect of montelukast in exercise-induced bronchoconstriction in children. Eur Respir J. 2006. 28:291–295.16. Busse WW, Lemanske RF Jr. Expert Panel Report 3: Moving forward to improve asthma care. J Allergy Clin Immunol. 2007. 120:1012–1014.17. Szefler SJ, Phillips BR, Martinez FD, Chinchilli VM, Lemanske RF, Strunk RC, Zeiger RS, Larsen G, Spahn JD, Bacharier LB, Bloomberg GR, Guilbert TW, Heldt G, Morgan WJ, Moss MH, Sorkness CA, Taussig LM. Characterization of within-subject responses to fluticasone and montelukast in childhood asthma. J Allergy Clin Immunol. 2005. 115:233–242.18. Zeiger RS, Szefler SJ, Phillips BR, Schatz M, Martinez FD, Chinchilli VM, Lemanske RF Jr, Strunk RC, Larsen G, Spahn JD, Bacharier LB, Bloomberg GR, Guilbert TW, Heldt G, Morgan WJ, Moss MH, Sorkness CA, Taussig LM. Childhood Asthma Research and Education Network of the National Heart, Lung, and Blood Institute. Response profiles to fluticasone and montelukast in mild-to-moderate persistent childhood asthma. J Allergy Clin Immunol. 2006. 117:45–52.19. Rabinovitch N, Graber NJ, Chinchilli VM, Sorkness CA, Zeiger RS, Strunk RC, Bacharier LB, Martinez FD, Szefler SJ. Childhood Asthma Research and Education Network of the National Heart, Lung, and Blood Institute. Urinary leukotriene E4/exhaled nitric oxide ratio and montelukast response in childhood asthma. J Allergy Clin Immunol. 2010. 126:545–551.e1-4.20. Rabinovitch N, Strand M, Stuhlman K, Gelfand EW. Exposure to tobacco smoke increases leukotriene E4-related albuterol usage and response to montelukast. J Allergy Clin Immunol. 2008. 121:1365–1371.21. Kharitonov SA, Yates D, Robbins RA, Logan-Sinclair R, Shinebourne EA, Barnes PJ. Increased nitric oxide in exhaled air of asthmatic patients. Lancet. 1994. 343:133–135.22. Massaro AF, Gaston B, Kita D, Fanta C, Stamler JS, Drazen JM. Expired nitric oxide levels during treatment of acute asthma. Am J Respir Crit Care Med. 1995. 152:800–803.23. Gogate S, Katial R. Pediatric biomarkers in asthma: exhaled nitric oxide, sputum eosinophils and leukotriene E4. Curr Opin Allergy Clin Immunol. 2008. 8:154–157.24. Crapo RO, Casaburi R, Coates AL, Enright PL, Hankinson JL, Irvin CG, MacIntyre NR, McKay RT, Wanger JS, Anderson SD, Cockcroft DW, Fish JE, Sterk PJ. Guidelines for methacholine and exercise challenge testing-1999. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. Am J Respir Crit Care Med. 2000. 161:309–329.25. Bateman ED, Hurd SS, Barnes PJ, Bousquet J, Drazen JM, FitzGerald M, Gibson P, Ohta K, O'Byrne P, Pedersen SE, Pizzichini E, Sullivan SD, Wenzel SE, Zar HJ. Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J. 2008. 31:143–178.26. Chai H, Farr RS, Froehlich LA, Mathison DA, McLean JA, Rosenthal RR, Sheffer AL, Spector SL, Townley RG. Standardization of bronchial inhalation challenge procedures. J Allergy Clin Immunol. 1975. 56:323–327.27. O'Sullivan S, Roquet A, Dahlén B, Dahlén S, Kumlin M. Urinary excretion of inflammatory mediators during allergen-induced early and late phase asthmatic reactions. Clin Exp Allergy. 1998. 28:1332–1339.28. Kumlin M, Stensvad F, Larsson L, Dahlén B, Dahlén SE. Validation and application of a new simple strategy for measurements of urinary leukotriene E4 in humans. Clin Exp Allergy. 1995. 25:467–479.29. Menzies D, Nair A, Lipworth BJ. Portable exhaled nitric oxide measurement: Comparison with the "gold standard" technique. Chest. 2007. 131:410–414.30. American Thoracic Society. European Respiratory Society. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am J Respir Crit Care Med. 2005. 171:912–930.31. Stelmach I, Grzelewski T, Majak P, Jerzynska J, Stelmach W, Kuna P. Effect of different antiasthmatic treatments on exercise-induced bronchoconstriction in children with asthma. J Allergy Clin Immunol. 2008. 121:383–389.32. Melo RE, Solé D, Naspitz CK. Exercise-induced bronchoconstriction in children: montelukast attenuates the immediate-phase and late-phase responses. J Allergy Clin Immunol. 2003. 111:301–307.33. Kim JH, Lee SY, Kim HB, Kim BS, Shim JY, Hong TJ, Hong SJ. Prolonged effect of montelukast in asthmatic children with exercise-induced bronchoconstriction. Pediatr Pulmonol. 2005. 39:162–166.34. Kemp JP, Dockhorn RJ, Shapiro GG, Nguyen HH, Reiss TF, Seidenberg BC, Knorr B. Montelukast once daily inhibits exercise-induced bronchoconstriction in 6- to 14-year-old children with asthma. J Pediatr. 1998. 133:424–428.35. Alexis NE, Hu SC, Zeman K, Alter T, Bennett WD. Induced sputum derives from the central airways: confirmation using a radiolabeled aerosol bolus delivery technique. Am J Respir Crit Care Med. 2001. 164:1964–1970.36. Freed AN, Wang Y, McCulloch S, Myers T, Suzuki R. Mucosal injury and eicosanoid kinetics during hyperventilation-induced bronchoconstriction. J Appl Physiol. 1999. 87:1724–1733.37. Hallstrand TS, Henderson WR Jr. Leukotriene modifiers. Med Clin North Am. 2002. 86:1009–1033. vi38. Mickleborough TD, Murray RL, Ionescu AA, Lindley MR. Fish oil supplementation reduces severity of exercise-induced bronchoconstriction in elite athletes. Am J Respir Crit Care Med. 2003. 168:1181–1189.39. Anderson SD, Brannan JD. Exercise-induced asthma: is there still a case for histamine? J Allergy Clin Immunol. 2002. 109:771–773.40. Yoshikawa T, Shoji S, Fujii T, Kanazawa H, Kudoh S, Hirata K, Yoshikawa J. Severity of exercise-induced bronchoconstriction is related to airway eosinophilic inflammation in patients with asthma. Eur Respir J. 1998. 12:879–884.41. Bonsignore MR, Morici G, Riccobono L, Insalaco G, Bonanno A, Profita M, Paternò A, Vassalle C, Mirabella A, Vignola AM. Airway inflammation in nonasthmatic amateur runners. Am J Physiol Lung Cell Mol Physiol. 2001. 281:L668–L676.42. Helenius I, Lumme A, Haahtela T. Asthma, airway inflammation and treatment in elite athletes. Sports Med. 2005. 35:565–574.43. Hermansen CL, Kirchner JT. Identifying exercise-induced bronchospasm. Treatment hinges on distinguishing it from chronic asthma. Postgrad Med. 2004. 115:15–16. 21–25.44. Sadeh J, Israel E. Airway narrowing in athletes: a different kettle of fish? Am J Respir Crit Care Med. 2003. 168:1146–1147.45. Holzer K, Anderson SD, Douglass J. Exercise in elite summer athletes: Challenges for diagnosis. J Allergy Clin Immunol. 2002. 110:374–380.46. Oh JW, Lee HB, Kang IJ, Kim SW, Park KS, Kook MH, Kim BS, Baek HS, Kim JH, Kim JK, Lee DJ, Kim KR, Choi YJ. The revised edition of korean calendar for allergenic pollens. Allergy Asthma Immunol Res. 2012. 4:5–11.47. Ahn SM, Rho HS, Baek HS, Joo YH, Hong YD, Shin SS, Park YH, Park SN. Inhibitory activity of novel kojic acid derivative containing trolox moiety on melanogenesis. Bioorg Med Chem Lett. 2011. 21:7466–7469.48. Yoon SH, Cho T, Kim HJ, Kim SY, Ko JH, Baek HS, Lee HJ, Lee CH. IVS6+5G>A found in Wiskott-Aldrich syndrome and X-linked thrombocytopenia in a Korean family. Pediatr Blood Cancer. 2012. 58:297–299.49. Pearlman DS, van Adelsberg J, Philip G, Tilles SA, Busse W, Hendeles L, Loeys T, Dass SB, Reiss TF. Onset and duration of protection against exercise-induced bronchoconstriction by a single oral dose of montelukast. Ann Allergy Asthma Immunol. 2006. 97:98–104.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Usefulness of Exhaled Nitric Oxide Test in Exercise-Induced Bronchoconstriction
- Nitric Oxide Correlates with Exercise-Induced Bronchoconstriction in Asthmatic Children
- Urinary N-methylhistamine and sulfidopeptide leukotriene in exercise-induced asthma
- Measurements of fractional exhaled nitric oxide in pediatric asthma
- Exercise induced delayed bronchoconstriction in children with asthma
