J Korean Med Sci.
2015 Jun;30(6):823-828. 10.3346/jkms.2015.30.6.823.
Single Center Experience of Five Diffuse Panbronchiolitis Patients Clinically Presenting as Severe Asthma
- Affiliations
-
- 1Department of Internal Medicine and Institute of Allergy, Yonsei University College of Medicine, Seoul, Korea. parkjw@yuhs.ac
- KMID: 2160614
- DOI: http://doi.org/10.3346/jkms.2015.30.6.823
Abstract
- Diffuse panbronchiolitis (DPB) is a bronchiolitis affecting the whole lung fields which can be treated by macrolide. Especially East Asian patients are more susceptible to diffuse panbronchiolitis. As asthma and DPB both can cause airway obstruction, differential diagnosis is important for the 2 diseases. Here we report 5 patients with DPB clinically presenting as severe asthma in Korea, who were well treated by macrolide. Among the 5 patients, 2 could stop their asthma inhalers and the other 3 could reduce asthma medications after diagnosis and treatment of DPB. In conclusion, considering DPB as differential diagnosis for asthmatics in Asian ethnic groups is important.
Keyword
MeSH Terms
-
Adult
Aged
Anti-Asthmatic Agents/*therapeutic use
Asthma/*diagnosis/*drug therapy
Bronchiolitis/*diagnosis/*drug therapy
Diagnosis, Differential
Female
Haemophilus Infections/*diagnosis/*drug therapy
Humans
Macrolides/*administration & dosage
Male
Middle Aged
Severity of Illness Index
Treatment Outcome
Anti-Asthmatic Agents
Macrolides
Figure
-

Fig. 1 Images of the Case 1. Initial chest x-ray showed bilateral haziness at bilateral lung field (A) and both maxillary sinusitis (B). Chest CT showed diffuse bronchial wall thickening with centrilobular nodules (C, D).

Fig. 2 Images of the Case 3. Bronchiolectasis and centrilobular nodules were observed on almost entire lung in his chest CT (A, B).
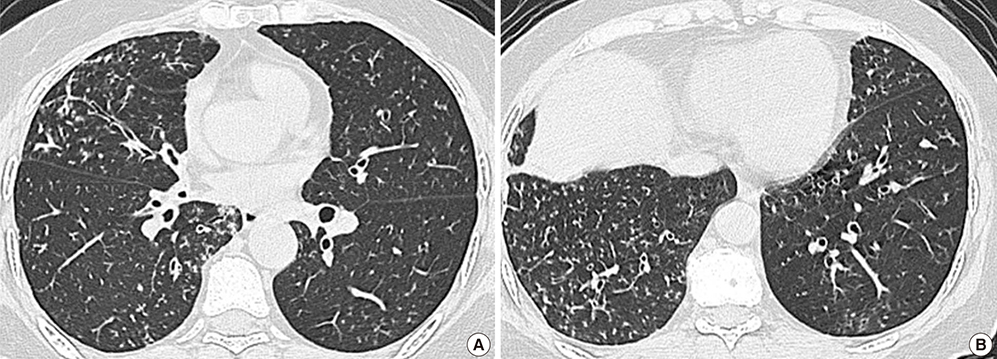
Fig. 3 Images of the Case 4. Initial CT showed bronchial wall thickening, centrilobular nodules (A, B).

Fig. 4 Images of the Case 5. Tiny nodules, bronchial wall thickening (A) and left maxillary sinusitis (B) were observed. Initial CT showed severe and diffuse centrilobular nodules (C). After treatment, multiple nodules were decreased (D).
Reference
-
1. Bateman ED, Hurd SS, Barnes PJ, Bousquet J, Drazen JM, FitzGerald M, Gibson P, Ohta K, O'Byrne P, Pedersen SE, et al. Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J. 2008; 31:143–178.2. Azuma A, Kudoh S. Diffuse panbronchiolitis in East Asia. Respirology. 2006; 11:249–261.3. Tsang KW, Ooi CG, Ip MS, Lam WK, Ngan H, Chan EY, Hawkins B, Ho CS, Amitani R, Tanaka E, et al. Clinical profiles of Chinese patients with diffuse panbronchiolitis. Thorax. 1998; 53:274–280.4. Matsuno O, Ueno K, Hayama Y, Honda H, Yamane H, Saeki Y. Deterioration of asthma in a patient with diffuse panbronchiolitis (DPB) after macrolide therapy. J Asthma. 2010; 47:486–488.5. Kadota J, Mukae H, Ishii H, Nagata T, Kaida H, Tomono K, Kohno S. Long-term efficacy and safety of clarithromycin treatment in patients with diffuse panbronchiolitis. Respir Med. 2003; 97:844–850.6. Poletti V, Casoni G, Chilosi M, Zompatori M. Diffuse panbronchiolitis. Eur Respir J. 2006; 28:862–871.7. Schultz MJ. Macrolide activities beyond their antimicrobial effects: macrolides in diffuse panbronchiolitis and cystic fibrosis. J Antimicrob Chemother. 2004; 54:21–28.8. Park HY, Suh GY, Chung MP, Kim H, Kwon OJ, Chung MJ, Kim TS, Lee KS, Koh WJ. Comparison of clinical and radiographic characteristics between nodular bronchiectatic form of nontuberculous mycobacterial lung disease and diffuse panbronchiolitis. J Korean Med Sci. 2009; 24:427–432.9. Kudoh S, Azuma A, Yamamoto M, Izumi T, Ando M. Improvement of survival in patients with diffuse panbronchiolitis treated with low-dose erythromycin. Am J Respir Crit Care Med. 1998; 157:1829–1832.10. Kanoh S, Rubin BK. Mechanisms of action and clinical application of macrolides as immunomodulatory medications. Clin Microbiol Rev. 2010; 23:590–615.11. Fujii T, Kadota J, Kawakami K, Iida K, Shirai R, Kaseda M, Kawamoto S, Kohno S. Long term effect of erythromycin therapy in patients with chronic Pseudomonas aeruginosa infection. Thorax. 1995; 50:1246–1252.12. Bisgaard H, Hermansen MN, Buchvald F, Loland L, Halkjaer LB, Bonnelykke K, Brasholt M, Heltberg A, Vissing NH, Thorsen SV, et al. Childhood asthma after bacterial colonization of the airway in neonates. N Engl J Med. 2007; 357:1487–1495.13. Marri PR, Stern DA, Wright AL, Billheimer D, Martinez FD. Asthma-associated differences in microbial composition of induced sputum. J Allergy Clin Immunol. 2013; 131:346–352.e1-3.14. Sethi S, Murphy TF. Infection in the pathogenesis and course of chronic obstructive pulmonary disease. N Engl J Med. 2008; 359:2355–2365.15. Wenzel RP, Fowler AA 3rd, Edmond MB. Antibiotic prevention of acute exacerbations of COPD. N Engl J Med. 2012; 367:340–347.16. Wallwork B, Coman W, Mackay-Sim A, Greiff L, Cervin A. A double-blind, randomized, placebo-controlled trial of macrolide in the treatment of chronic rhinosinusitis. Laryngoscope. 2006; 116:189–193.17. Hansen CR, Pressler T, Hoiby N, Johansen HK. Long-term, low-dose azithromycin treatment reduces the incidence but increases macrolide resistance in Staphylococcus aureus in Danish CF patients. J Cyst Fibros. 2009; 8:58–62.18. Phaff SJ, Tiddens HA, Verbrugh HA, Ott A. Macrolide resistance of Staphylococcus aureus and Haemophilus species associated with long-term azithromycin use in cystic fibrosis. J Antimicrob Chemother. 2006; 57:741–746.
