Radiological Evaluation and Classification of Adult Spinal Deformity
- Affiliations
-
- 1Department of Orthopedic Surgery, Inha University School of Medicine, Incheon, Korea. chokj@inha.ac.kr
- KMID: 2154344
- DOI: http://doi.org/10.4055/jkoa.2016.51.1.1
Abstract
- As the elderly population increases, the number of adult spinal deformity patients is also increasing. Unlike the main symptom of adolescent deformity is deformity itself, the symptoms of adult spinal deformity are various such as back pain and radiating pain to the extremities, which are associated with degenerative change. Deformities also show various combinations of scoliosis, kyphosis, coronal and sagittal imbalances. Various symptoms and complex deformities as well as old ages make treatment of the adult spinal deformity difficult. Radiographs of the spinal deformity should include spine and pelvis and hip joints in long films. Spinal deformity is influenced by regional curve, rotation of pelvis, and positions of hip and knee joints. The pelvis is a key structure in regulating spinal balances. Pelvic incidence, pelvic tilt and sacral slope are the most widely used spino-pelvic parameters. Pelvic incidence is fixed constant, which is unchanged when bone growth is complete. Pelvic incidence has a positive correlation with lumbar lordosis, and serves as a reference value in determining how much correction of lumbar lordosis is required in patients with sagittal imbalance. More correction of lumbar lordosis is required in patients with higher pelvic incidence. In order to maintain spinal balance, the combination of thoracic kyphosis, lumbar lordosis, and pelvic tilt should be harmonized. In particular, the match of pelvic incidence and lumbar lordosis is important to maintaining a balanced spine.
MeSH Terms
Figure
-

Figure 1 Coronal and sagittal imbalance. Coronal imbalance is defined as the C7 plumb line passes >2.5 cm lateral from the central sacral line. Sagittal imbalance is defined as the C7 plumb line passes >5 cm anterior from the posterosuperior corner of the sacrum.

Figure 2 Compensatory mechanism of sagittal imbalance. Data from the article of Cho et al. (Spine (Phila Pa 1976). 2013;38:E1561-6).8) (A) Neutral sagittal balance shows harmonious thoracic kyphosis and lumbar lordosis. Sacral slope is approximately 30°. (B) Loss of lordosis due to hypolordotic fusion in the lower lumbar spine leads to positive sagittal imbalance. (C) With a compensatory mechanism, hyperextending disc space at mobile segments can cause the C7 plumb line to be restored to the near normal range. (D) As patients grow older, subsequent disc degeneration develops at the mobile segments and then sagittal imbalance develops again. (E) Compensatory retroversion of the pelvis produces a vertical sacrum and reestablishes sagittal balance. Sacral slope is approximately 0°.

Figure 3 Spino-pelvic parameter. Pelvic incidence (PI) is the sum of pelvic tilt (PT) and sacral slope (SS). Normal ranges of these parameters are wide, so that the combination of them is more affected than the individual value.

Figure 4 (A, B) Both radiographs show same SVA. (A) Pelvic tilt is 57°, showing severe retroversion of the pelvis, which is associated with compensation for the sagittal imbalance. (B) Pelvic tilt is normal range which means no retroversion of the pelvis. SVA, sagittal vertical axis; LL, lumbar lordosis; SS, sacral slope; PI, pelvic incidence; PT, pelvic tilt.
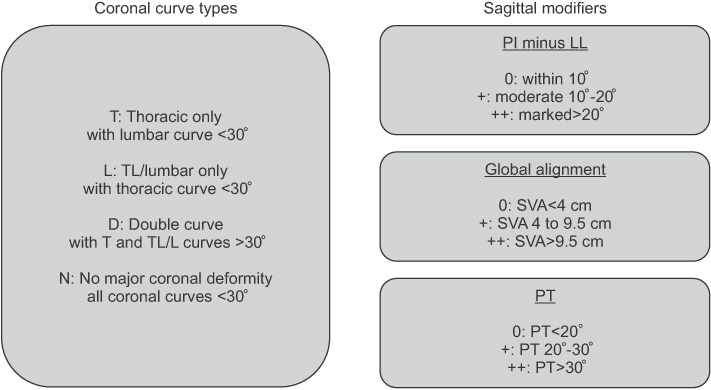
Figure 5 Scoliosis Research Society-Schwab classification of adult spinal deformity. Data from the article of Schwab et al. (Spine (Phila Pa 1976). 2012;37:1077-82).20) PI, pelvic incidence; LL, lumbar lordosis; SVA, sagittal vertical axis; PT, pelvic tilt.
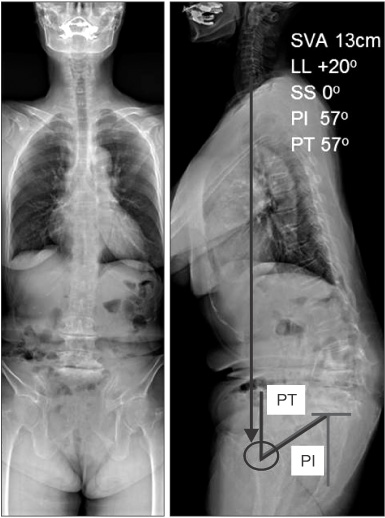
Figure 6 This 72-year-old female showed degenerative sagittal imbalance, 13 cm of sagittal vertical axis (SVA). On the radiographs, lumbar lordosis (LL) was kyphosis +21°, pelvic incidence (PI) was 57°, and pelvic tilt (PT) was 57°. According to the Scoliosis Research Society-Schwab classification, coronal curve type is N, and all sagittal modifiers were found ++ in PI-LL, SVA, and PT. This patient underwent pedicle subtraction osteotomy at L3, and posterior instrumentation from T12 to S1 with iliac screw fixation. SS, sacral slope.
Reference
-
1. Cho KJ, Kim YT, Shin SH, Suk SI. Surgical treatment of adult degenerative scoliosis. Asian Spine J. 2014; 8:371–381.
Article2. Lee CS, Chung SS, Kang KC, Park SJ, Shin SK. Normal patterns of sagittal alignment of the spine in young adults radiological analysis in a Korean population. Spine (Phila Pa 1976). 2011; 36:E1648–E1654.
Article3. Jackson RP, McManus AC. Radiographic analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex, and size. A prospective controlled clinical study. Spine (Phila Pa 1976). 1994; 19:1611–1618.4. Bernhardt M, Bridwell KH. Segmental analysis of the sagittal plane alignment of the normal thoracic and lumbar spines and thoracolumbar junction. Spine (Phila Pa 1976). 1989; 14:717–721.
Article5. Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976). 2005; 30:2024–2029.
Article6. Booth KC, Bridwell KH, Lenke LG, Baldus CR, Blanke KM. Complications and predictive factors for the successful treatment of flatback deformity (fixed sagittal imbalance). Spine (Phila Pa 1976). 1999; 24:1712–1720.
Article7. Lagrone MO, Bradford DS, Moe JH, Lonstein JE, Winter RB, Ogilvie JW. Treatment of symptomatic flatback after spinal fusion. J Bone Joint Surg Am. 1988; 70:569–580.
Article8. Cho KJ, Kim KT, Kim WJ, et al. Pedicle subtraction osteotomy in elderly patients with degenerative sagittal imbalance. Spine (Phila Pa 1976). 2013; 38:E1561–E1566.
Article9. Lee CS, Lee CK, Kim YT, Hong YM, Yoo JH. Dynamic sagittal imbalance of the spine in degenerative flat back: significance of pelvic tilt in surgical treatment. Spine (Phila Pa 1976). 2001; 26:2029–2035.10. During J, Goudfrooij H, Keessen W, Beeker TW, Crowe A. Toward standards for posture. Postural characteristics of the lower back system in normal and pathologic conditions. Spine (Phila Pa 1976). 1985; 10:83–87.11. Duval-Beaupère G, Schmidt C, Cosson P. A barycentremetric study of the sagittal shape of spine and pelvis: the conditions required for an economic standing position. Ann Biomed Eng. 1992; 20:451–462.
Article12. Mendoza-Lattes S, Ries Z, Gao Y, Weinstein SL. Natural history of spinopelvic alignment differs from symptomatic deformity of the spine. Spine (Phila Pa 1976). 2010; 35:E792–E798.
Article13. Legaye J, Duval-Beaupère G, Hecquet J, Marty C. Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J. 1998; 7:99–103.
Article14. Schwab FJ, Patel A, Shaffrey CI, et al. Sagittal realignment failures following pedicle subtraction osteotomy surgery: are we doing enough?: clinical article. J Neurosurg Spine. 2012; 16:539–546.15. Cho KJ, Suk SI, Park SR, et al. Risk factors of sagittal decompensation after long posterior instrumentation and fusion for degenerative lumbar scoliosis. Spine (Phila Pa 1976). 2010; 35:1595–1601.
Article16. Aebi M. The adult scoliosis. Eur Spine J. 2005; 14:925–948.
Article17. Lowe T, Berven SH, Schwab FJ, Bridwell KH. The SRS classification for adult spinal deformity: building on the King/Moe and Lenke classification systems. Spine (Phila Pa 1976). 2006; 31:19 Suppl. S119–S125.18. Schwab F, Farcy JP, Bridwell K, et al. A clinical impact classification of scoliosis in the adult. Spine (Phila Pa 1976). 2006; 31:2109–2114.
Article19. Schwab F, Lafage V, Farcy JP, et al. Surgical rates and operative outcome analysis in thoracolumbar and lumbar major adult scoliosis: application of the new adult deformity classification. Spine (Phila Pa 1976). 2007; 32:2723–2730.20. Schwab F, Ungar B, Blondel B, et al. Scoliosis Research Society-Schwab adult spinal deformity classification: a validation study. Spine (Phila Pa 1976). 2012; 37:1077–1082.21. Schwab FJ, Blondel B, Bess S, et al. International Spine Study Group (ISSG). Radiographical spinopelvic parameters and disability in the setting of adult spinal deformity: a prospective multicenter analysis. Spine (Phila Pa 1976). 2013; 38:E803–E812.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Decision Making Algorithm for Adult Spinal Deformity Surgery
- Cervical Deformity: Evaluation, Classification, and Surgical Planning
- Minimally Invasive Spinal Surgery for Adult Spinal Deformity
- What Should an Ideal Adult Spinal Deformity Classification System Consist of?: Review of the Factors Affecting Outcomes of Adult Spinal Deformity Management
- From the Spinopelvic Parameters to Global Alignment and Proportion Scores in Adult Spinal Deformity
