Ewha Med J.
2016 Jan;39(1):23-27. 10.12771/emj.2016.39.1.23.
Tocilizumab-induced Transaminitis in a Seropositive Rheumatoid Arthritis Patient with Macrophage Activation Syndrome
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. sangwonlee@yuhs.ac
- KMID: 2152754
- DOI: http://doi.org/10.12771/emj.2016.39.1.23
Abstract
- As a new humanized monoclonal antibody against the interleukin-6 receptor, tocilizumab is currently used for the treatment of rheumatoid arthritis (RA) patients. Tocilizumab was reported to provoke drug-related liver toxicity, although there have been no reports on significant liver toxicity from tocilizumab in Korean patients with RA to date. Here, we describe the first case of tocilizumab-related liver toxicity in a patient with complicated RA, accompanied with macrophage activation syndrome, who had received tacrolimus and prednisolone and in whom both conventional disease modifying anti-rheumatic drugs, including methotrexate, leflunomide and sulfasalazine or tumor necrotizing factor-alpha blockades, were contraindicated due to drug eruption and a history of lung cancer.
Keyword
MeSH Terms
-
Antirheumatic Agents
Arthritis, Rheumatoid*
Drug Eruptions
Humans
Interleukin-6
Liver
Lung Neoplasms
Macrophage Activation Syndrome*
Macrophage Activation*
Macrophages*
Methotrexate
Prednisolone
Sulfasalazine
Tacrolimus
Tranexamic Acid*
Antirheumatic Agents
Interleukin-6
Methotrexate
Prednisolone
Sulfasalazine
Tacrolimus
Tranexamic Acid
Figure
-
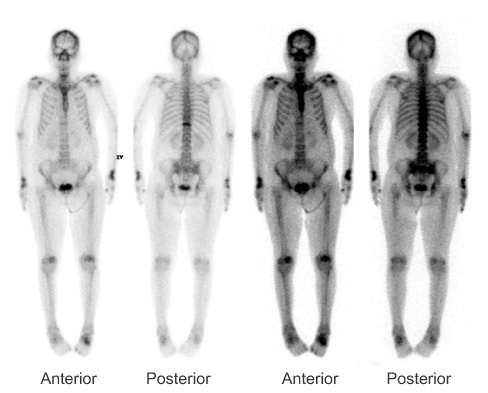
Fig. 1 Whole body bone scan. It reveals increased uptake in the bilateral wrists, hands, and left tarsal bone, areas of arthritis.
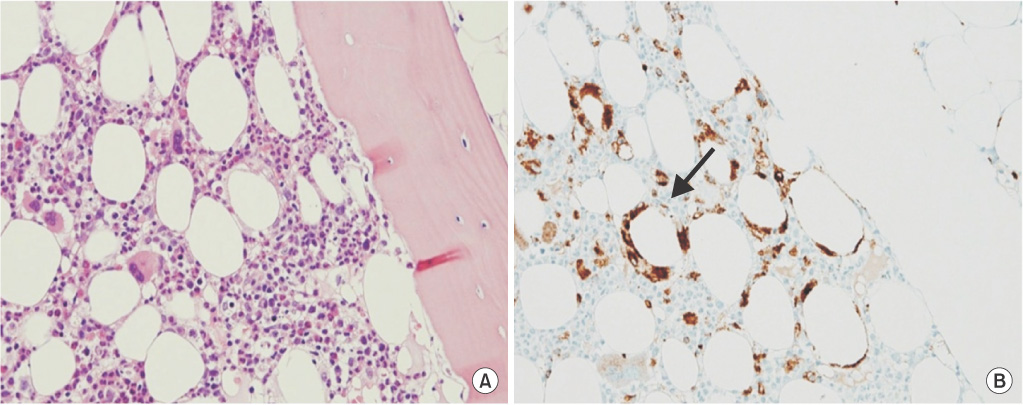
Fig. 2 Bone marrow biopsy pathology and immunohistochemical staining of macrophage. It demonstrates areas of fat necrosis surrounded by macrophages (A), which shows CD68 positivity on immunohistochemical staining (B, arrow) (A: H&E, ×200; B: CD68 immunohistochemical stain, ×200).
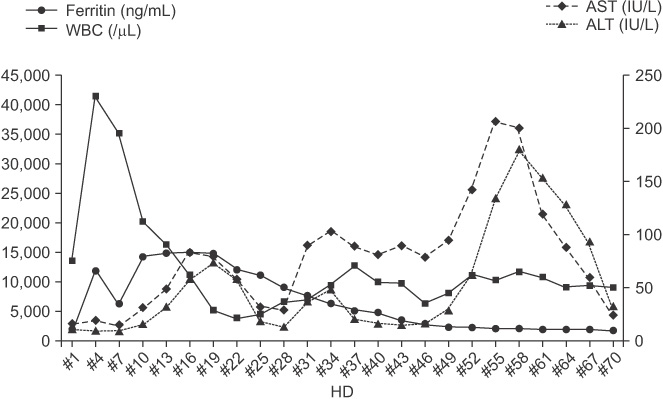
Fig. 3 The graph of the trend of changes in liver enzyme, WBC, and ferritin during tocilizumab treatment. While ferritin and WBC decreases after tocilizumab administration, there is an increase in the liver enzyme. AST, aspartate aminotransferase; ALT, alanine aminotransferase; HD, hospital day; WBC, white blood cell.
Reference
-
1. Emery P, Keystone E, Tony HP, Cantagrel A, van Vollenhoven R, Sanchez A, et al. IL-6 receptor inhibition with tocilizumab improves treatment outcomes in patients with rheumatoid arthritis refractory to anti-tumour necrosis factor biologicals: results from a 24-week multicentre randomised placebo-controlled trial. Ann Rheum Dis. 2008; 67:1516–1523.2. Genovese MC, McKay JD, Nasonov EL, Mysler EF, da Silva NA, Alecock E, et al. Interleukin-6 receptor inhibition with tocilizumab reduces disease activity in rheumatoid arthritis with inadequate response to disease-modifying antirheumatic drugs: the tocilizumab in combination with traditional disease-modifying antirheumatic drug therapy study. Arthritis Rheum. 2008; 58:2968–2980.3. Maini RN, Taylor PC, Szechinski J, Pavelka K, Broll J, Balint G, et al. Double-blind randomized controlled clinical trial of the interleukin-6 receptor antagonist, tocilizumab, in European patients with rheumatoid arthritis who had an incomplete response to methotrexate. Arthritis Rheum. 2006; 54:2817–2829.4. Jones G, Sebba A, Gu J, Lowenstein MB, Calvo A, Gomez-Reino JJ, et al. Comparison of tocilizumab monotherapy versus methotrexate monotherapy in patients with moderate to severe rheumatoid arthritis: the AMBITION study. Ann Rheum Dis. 2010; 69:88–96.5. Smolen JS, Beaulieu A, Rubbert-Roth A, Ramos-Remus C, Rovensky J, Alecock E, et al. Effect of interleukin-6 receptor inhibition with tocilizumab in patients with rheumatoid arthritis (OPTION study): a double-blind, placebo-controlled, randomised trial. Lancet. 2008; 371:987–997.6. Ravelli A, Magni-Manzoni S, Pistorio A, Besana C, Foti T, Ruperto N, et al. Preliminary diagnostic guidelines for macrophage activation syndrome complicating systemic juvenile idiopathic arthritis. J Pediatr. 2005; 146:598–604.7. Alfreijat M, Habibi M, Bhatia P, Bhatia A. Severe hepatitis associated with tocilizumab in a patient with rheumatoid arthritis. Rheumatology (Oxford). 2013; 52:1340–1341.8. Mahamid M, Paz K, Reuven M, Safadi R. Hepatotoxicity due to tocilizumab and anakinra in rheumatoid arthritis: two case reports. Int J Gen Med. 2011; 4:657–660.9. Kovalovich K, DeAngelis RA, Li W, Furth EE, Ciliberto G, Taub R. Increased toxin-induced liver injury and fibrosis in interleukin-6-deficient mice. Hepatology. 2000; 31:149–159.10. Drepper M, Rubbia-Brandt L, Spahr L. Tocilizumab-induced acute liver injury in adult onset Still's disease. Case Reports Hepatol. 2013; 2013:964828.11. Schiff MH, Kremer JM, Jahreis A, Vernon E, Isaacs JD, van Vollenhoven RF. Integrated safety in tocilizumab clinical trials. Arthritis Res Ther. 2011; 13:R141.12. Kobayashi M, Takahashi Y, Yamashita H, Kaneko H, Mimori A. Benefit and a possible risk of tocilizumab therapy for adult-onset Still's disease accompanied by macrophage-activation syndrome. Mod Rheumatol. 2011; 21:92–96.13. Deane S, Selmi C, Teuber SS, Gershwin ME. Macrophage activation syndrome in autoimmune disease. Int Arch Allergy Immunol. 2010; 153:109–120.14. Arico M, Danesino C, Pende D, Moretta L. Pathogenesis of haemophagocytic lymphohistiocytosis. Br J Haematol. 2001; 114:761–769.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Sepsis Caused by Cellulitis in a Patient with Rheumatoid Arthritis after Tocilizumab Treatment
- Drug retention of biologic and targeted synthetic disease-modifying antirheumatic drugs in Korean patients with seropositive rheumatoid arthritis
- Acute Ischemic Stroke in the Patients with Inflammatory Arthritis: An Analysis of Data from National Health Insurance Service
- Macrophage Activation Syndrome in Juvenile Rheumatoid Arthritis Successfully Treated with Cyclosporine A: A Case Report
- A Case of Gold Induced Hypersensitivity Pneumonitis Diagnosed by Lymphocyte Stimulation Test with Gold
