Isolated Myeloid Sarcoma Presenting as Cord Compression by Paraspinal Mass
- Affiliations
-
- 1Department of Internal Medicine, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea. yjyuh@paik.ac.kr
- 2Department of Pathology, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea.
- 3Department of Laboratory Medicine, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea.
- KMID: 2152753
- DOI: http://doi.org/10.12771/emj.2016.39.1.17
Abstract
- Myeloid sarcoma is a rare tumor mass consisting of immature granulocytic cells occurring in an extramedullary site or in a bone. It has often been observed during the course of an acute leukemia, myelodysplastic syndrome or myeloproliferative neoplasms, and it can involve any site of the body. However, it rarely present in the absence of bone marrow infiltration, especially for the isolated spinal myeloid sarcoma. In this report, we describe a case of isolated myeloid sarcoma that showed spinal compression. A 66-year-old male, with no underlying disease or medication history, presented with a progressive back pain and numbness in bilateral lower extremities that had begun two weeks before. He was diagnosed with myeloid sarcoma with no evidence of bone marrow involvement. Tumor cells were positive for CD34, c-KIT, and Bcl-2 on the immunohistochemical stain. He was treated with systemic chemotherapy with daunorubicin plus cytosine arabinoside and achieved a partial response.
Keyword
MeSH Terms
Figure
-
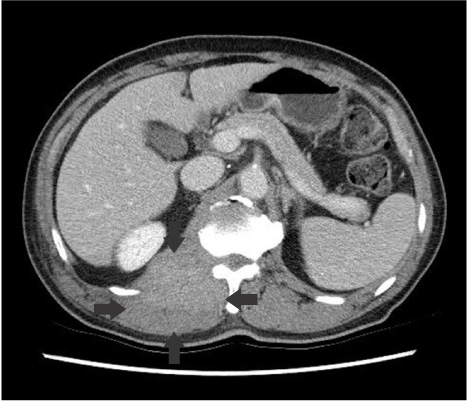
Fig. 1 Computed tomography on admission. It shows extension of right paraspinal mass (arrows) into epidural space.
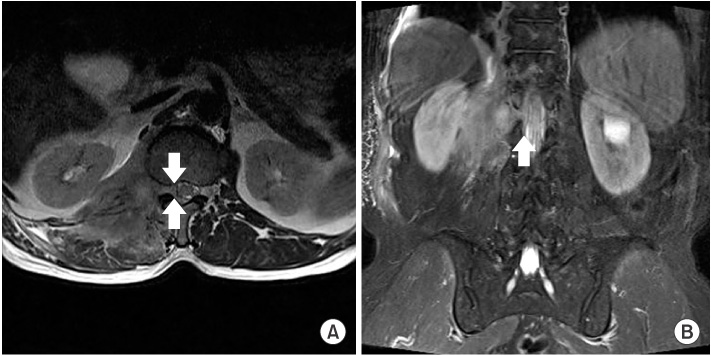
Fig. 2 Magnetic resonance (MR) image of the spine. (A) Axial T2-weighted MR image and (B) coronal T2-weighted fatsaturated MR image show epidural spinal cord compression (arrows).
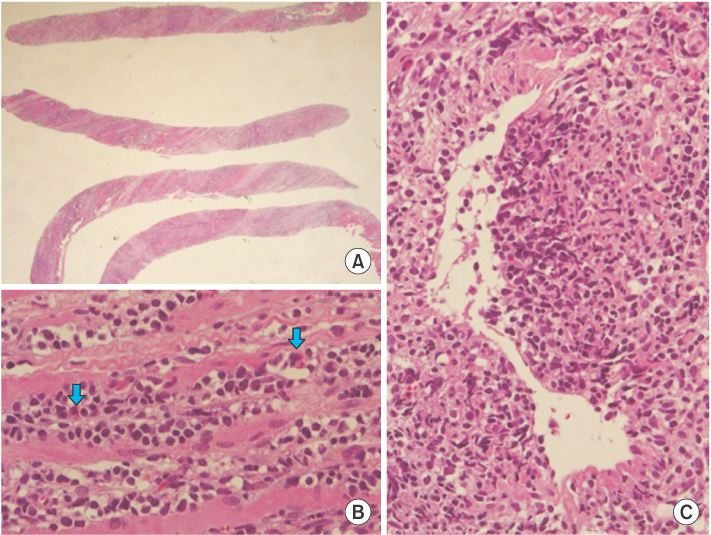
Fig. 3 Histologic finding of psoas muscle core-needle biopsy. (A) The sections show 4 cores of needle biopsied specimen (H&E, ×10). (B) High power field reveals small round blue cells infiltrating into skeletal muscle fibers. Some cells with eosinophilic granules (arrows) are also found, suggestive of immature blasts of eosinophil (H&E, ×400). (C) The tumor cells infiltrates into venous wall with partial disruption (H&E, ×200).
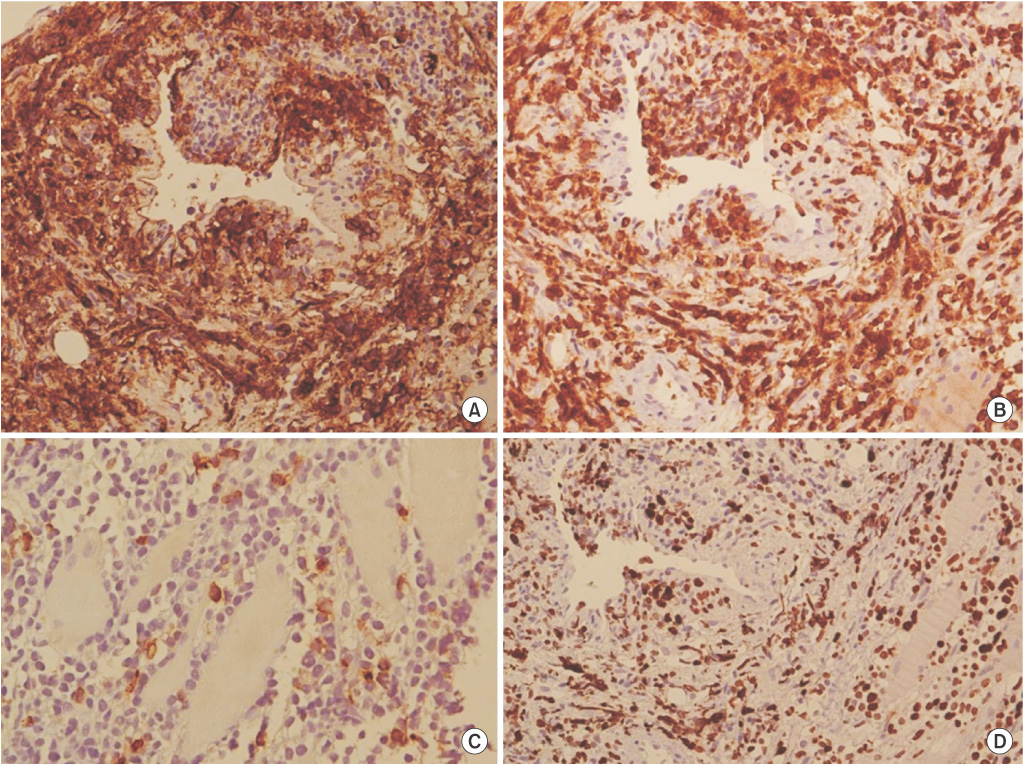
Fig. 4 Immunohistochemical staining for tumor. (A) CD34 is positive for tumor cells (×200). (B) Bcl-2 is positive for tumor cells (×200). (C) C-KIT is focal positive (×200). (D) The percentage of Ki-67 positive cells is 70% (×200).
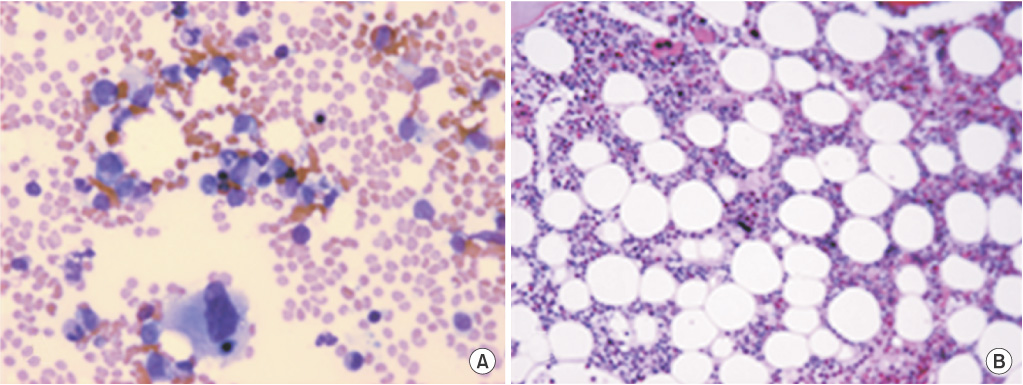
Fig. 5 Bone marrow aspirates and biopsy findings. (A) Hematopoietic cells of three lineages are within normal limit in number and distribution. No malignant cells are observed (Wright-Giemsa, ×400). (B) Bone marrow biopsy shows normocellular marrow. Hematopoietic cells of three lineages are within normal limit in number and distribution. No malignant cells are observed (H&E, ×100).
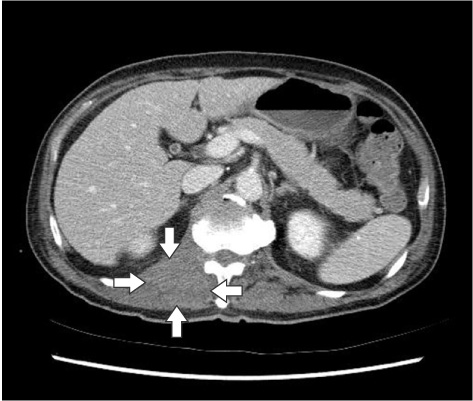
Fig. 6 A follow-up computed tomography. It shows a decreased extent of enhancing right paraspinal mass (arrows).
Reference
-
1. Yilmaz AF, Saydam G, Sahin F, Baran Y. Granulocytic sarcoma: a systematic review. Am J Blood Res. 2013; 3:265–270.2. Desplechin A, Mekinian A, Rossignol J, Denis G, Gosset P, Cambier N, et al. Isolated megakaryoblastic bone sarcoma revealing acute myeloproliferative syndrome. Joint Bone Spine. 2010; 77:277–278.3. Bakst RL, Tallman MS, Douer D, Yahalom J. How I treat extramedullary acute myeloid leukemia. Blood. 2011; 118:3785–3793.4. Avni B, Koren-Michowitz M. Myeloid sarcoma: current approach and therapeutic options. Ther Adv Hematol. 2011; 2:309–316.5. Chargari C, Jacob J, Bauduceau O, Ferrand FR, De Revel T, Vedrine L. Granulocytic sarcoma in a nonleukemic patient: place of radiotherapy and systemic therapies. Case Rep Med. 2011; 2011:929161.6. Kalayci M, Sumer M, Yenidunya S, Ozdolap S, Acikgoz B. Spinal granulocytic sarcoma (chloroma) presenting as acute cord compression in a nonleukemic patient. Neurol India. 2005; 53:221–223.7. Shiozawa Y, Kiyokawa N, Saito M, Fujimoto J, Hata J, Yamashiro Y. Granulocytic sarcoma of the spine in a child without bone marrow involvement: a case report and literature review. Eur J Pediatr. 2005; 164:616–620.8. Tsimberidou AM, Kantarjian HM, Estey E, Cortes JE, Verstovsek S, Faderl S, et al. Outcome in patients with nonleukemic granulocytic sarcoma treated with chemotherapy with or without radiotherapy. Leukemia. 2003; 17:1100–1103.9. Yamauchi K, Yasuda M. Comparison in treatments of nonleukemic granulocytic sarcoma: report of two cases and a review of 72 cases in the literature. Cancer. 2002; 94:1739–1746.10. Antic D, Elezovic I, Milic N, Suvajdzic N, Vidovic A, Perunicic M, et al. Is there a "gold" standard treatment for patients with isolated myeloid sarcoma? Biomed Pharmacother. 2013; 67:72–77.11. Imrie KR, Kovacs MJ, Selby D, Lipton J, Patterson BJ, Pantalony D, et al. Isolated chloroma: the effect of early antileukemic therapy. Ann Intern Med. 1995; 123:351–353.12. Inoue T, Takahashi T, Shimizu H, Kanamori M, Kumabe T, Watanabe M, et al. Spinal granulocytic sarcoma manifesting as radiculopathy in a nonleukemic patient. Neurol Med Chir (Tokyo). 2008; 48:131–136.13. Lee KH, Kim H, Choi GY, Lee JH, Han HS, Lee KH, et al. Granulocytic sarcoma presenting in two patients without leukemia. Korean J Med. 2009; 77:236–240.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Granulocytic sarcoma presenting in two patients without leukemia
- Clinical Experience of Leukemia with Extradural Chloroma during Treatment of Lower Back Pain
- Isolated Myeloid Sarcoma in the Nasal Cavity Without Bone Marrow Involvement in a 5-Year-Old Child
- A Case of Granulocytic Sarcoma causing Spinal Cord Compression in Chronic Myelogenous Leukemia
- Granulocyte sarcoma as a presenting spinal cord compression
