J Korean Soc Spine Surg.
2015 Dec;22(4):170-177. 10.4184/jkss.2015.22.4.170.
Restoration of Segmental Lordosis and Related Factors in Interbody Fusion for Degenerative Lumbar Disease
- Affiliations
-
- 1Department of Orthopaedic Surgery, College of Medicine, Soonchunhyang University Bucheon Hospital, Korea. eungha@gmail.com
- KMID: 2150545
- DOI: http://doi.org/10.4184/jkss.2015.22.4.170
Abstract
- STUDY DESIGN: A retrospective study.
OBJECTIVES
To analyze restoration of segmental lordosis and factors related to interbody fusion and the fusion rate with degenerative lumbar disease. SUMMARY OF LITERATURE REVIEW: Few studies have addressed the restoration of segmental lordosis and factors related to interbody fusion for degenerative lumbar disease.
MATERIALS AND METHODS
Records of 43 patients treated by anterior lumbar interbody fusion (ALIF) or posterior lumbar interbody fusion (PLIF) surgery from 2011 to 2013 were reviewed. ALIF used a metal cage with a 10degrees lordotic angle and PLIF used a metal cage with an 8degrees lordotic angle. Preoperative, postoperative, and at least 1 year outcomes were analyzed from radiographs. As a related factor, segmental flexibility, disc height, osteophytes, vaccuum disc, hypertrophic facet, spondylolisthesis, and endplate violation were analyzed. We also analyzed the bony union rate.
RESULTS
The segmental lordotic angle was 4.67degrees before surgery, improved to 10.43degrees after surgery, and was 9.32degrees at the final follow-up. Comparing between the ALIF and PLIF at the L3-4 level in a similar number of patients revealed 7.24degrees and 4.61degrees restoration after ALIF and PLIF surgery, postoperatively. The difference was statistically significant (p=0.011). Segmental flexibility had a statistically significant positive correlation (p=0.013). Lower disc height and osteophytes limited restoration of segmental lordosis, but vaccuum disc was restored well after interbody fusion. Bony union was achieved in 92.8% of the cases.
CONCLUSIONS
Intebody fusion, especially ALIF surgery, results in acceptable restoration of segmental lordosis. Even with narrowed disc space or osteophytes, remained segmental flexibility is an important factor of segmental lordosis restoration.
Keyword
MeSH Terms
Figure
-

Fig. 1. The segmental angle is between the lower endplate of the upper vertebra body and upper endplate of the lower vertebra body. (A) preoperative, (B) postoperative.
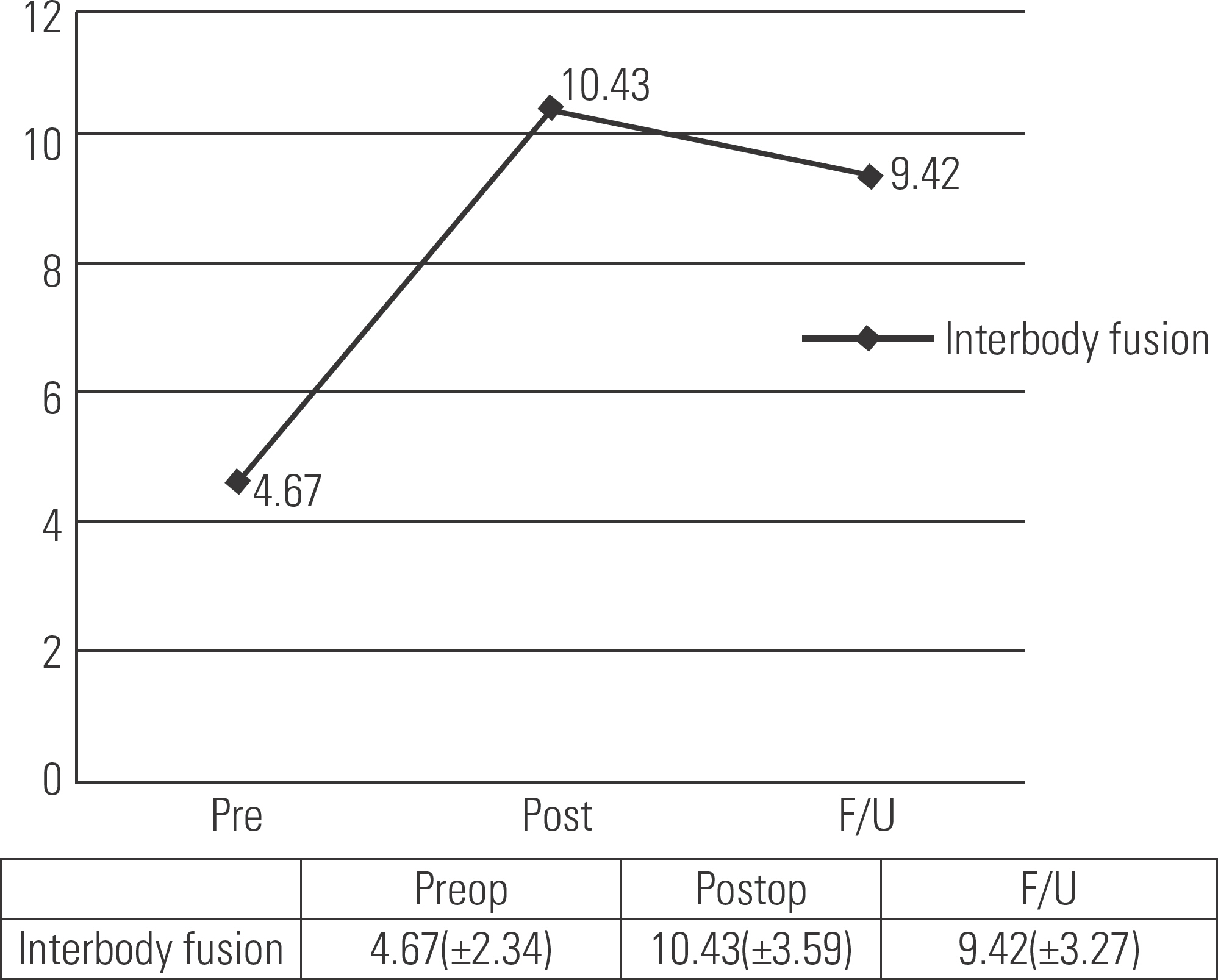
Fig. 2. The segmental lordosis angle was well restored after interbody fusion surgery.

Fig. 3. The segmental lordosis angle was restored more successfully after ALIF surgery than PLIF surgery at the same L3-4 level.
Reference
-
1. Lee CS, Kim YT, Kim EG. Clinical study of lumbar degenerative kphosis. J Korean Soc Spine Surg. 1997; 4:27–35.2. Becker's L, Bekaert J. The role of lordosis. Acta Orthop Belg. 1991; 57(Suppl):198–202.3. Diedrich O, Perlick L, Schmitt O, et al. Radiographic spinal profile changes induced by cage design after posterior lumbar interbody fusion. Preliminary report of a study with wedged implants. Spine (Phila Pa 1976). 2001; 26:E274–80.4. Cho KJ, Kim KT, Kim WJ, et al. Pedicle subtraction osteot-omy in elderly patients with degenerative sagittal imbalance. Spine (Phila Pa 1976). 2013; 38:E1561–6.
Article5. Lagrone MO, Bradford DS, Moe JH, et al. Treatment of symptomatic flatback after spinal fusion. J Bone Joint Surg Am. 1988; 70:569–80.
Article6. Liebensteiner MC, Jesacher G, Thaler M, et al. Restoration and preservation of disc height and segmental lordosis with circumferential lumbar fusion: a retrospective analysis of cage versus bone graft. J Spinal Disord Tech. 2011; 24:44–9.7. Pathria M, Sartoris DJ, Resnick D. Osteoarthritis of the facet joints: accuracy of oblique radiographic assessment. Radi-ology. 1987; 164:227–30.
Article8. Brantigan JW, Steffee AD, Geiger JM. A carbon fiber im-plant to aid interbody fusion. Mechanical testing. Spine (Phila Pa 1976). 1991; 16(Suppl):277–82.9. Brantigan JW, Steffee AD, Lewis ML, et al. Lumbar interbody fusion using the Brantigan I/F cage for posterior lumbar interbody fusion and the variable pedicle screw placement system: two-year results from a Food and Drug Administration investigational device exemption clinical trial. Spine (Phila Pa 1976). 2000; 25:1437–46.10. Deyo RA, Ciol MA, Cherkin DC, et al. Lumbar spinal fusion. A cohort study of complications, reoperations, and resource use in the Medicare population. Spine (Phila Pa 1976). 1993; 18:1463–70.11. Kim JH, Kim SS, Kim JH, et al. Comparison of monosegment instrumented posterior lumbar interbody fusion with and without a metal cage in degenerative spine. J Korean Orthop Assoc. 2008; 43:143–51.
Article12. Song KJ, Lim YJ, Choi BW, et al. Clinical efficacy of a stand-alone, threaded-titanium fusion cage for single-level degenerative lumbar spinal disorders. J Korean Orthop Assoc. 2008; 43:152–9.
Article13. Takahashi H, Suguro T, Yokoyama Y, et al. Effect of cage geometry on sagittal alignment after posterior lumbar interbody fusion for degenerative disc disease. J Orthop Surg (Hong Kong). 2010; 18:139–42.
Article14. Capener N. Spondylolithesis. Br J Surg. 1932; 19:374–80.15. Lane JD, Moore ES. Transperitoenal approach to the intervertebral disc in the lumbar area. Ann Surg. 1948; 127:537–42.16. Harmon PH. Anterior excision and vertebral body fusion operation for intervertebral disc syndromes of the lower lumbar spine: Three to five-year results in 244 cases. Clin Orthop. 1963; 26:107–18.17. Goldner JL, Urbaniak JR, McCollumn DE. Anterior disc excision and interbody spinal fusion for chronic low back pain. Orthop Clin North Am. 1971; 2:543–52.
Article18. Sacks S. Anterior interbody fusion of the lumbar spine. J Bone Joint Surg Br. 1965; 47:211–23.
Article19. Stonecipher T, Wright S. Posterior lumbar interbody fusion with facet-screw fixation. Spine (Phila Pa 1976). 1989; 14:468–71.
Article20. Yoon YH, Cho KJ, Park SR, et al. Posterior lumbar interbody fusion and unilateral posterolateral fusion with local bone and single cage: comparison with posterolateral lumbar fusion and autologous iliac bone. J Korean Orthop Assoc. 2009; 44:102–8.21. Lazennec JY, Ramaré S, Arafati N, et al. Sagittal alignment in lumbosacral fusion: relations between radiological parameters and pain. Eur Spine J. 2000; 9:47–55.
Article22. Kumar MN, Baklanov A, Chopin D. Correlation between-sagittal plane changes and adjacent segment degeneration following lumbar spine fusion. Eur Spine J. 2001; 10:314–9.23. Lafage V, Schwab F, Skalli W, et al. Standing balance and sagittal plane spinal deformity: analysis of spinopelvic and gravity line parameters. Spine (Phila Pa 1976). 2008; 33:1572–8.24. Hashimoto T, Shigenobu K, Kanayama M, et al. Clinical results of single-level posterior lumbar interbody fusion using the Brantigan I/F carbon cage filled with a mixture of local morselized bone and bioactive ceramic granules. Spine (Phila Pa 1976). 2002; 27:258–62.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Lumbar Lordosis Restoration with an Eight Degree Cage in Posterior Lumbar Interbody Fusion for Lumbar Degenerative Disease
- Restoration of Lumbar Lordosis After Posterior Lumbar Interbody Fusion with 4 Degree Cage in Degenerative Spinal Disease
- Radiographic Results of Single Level Transforaminal Lumbar Interbody Fusion in Degenerative Lumbar Spine Disease: Focusing on Changes of Segmental Lordosis in Fusion Segment
- A Comparative Study of Lateral Lumbar Interbody Fusion and Posterior Lumbar Interbody Fusion in Degenerative Lumbar Spondylolisthesis
- Factors Affecting Segmental Lordotic Angle After Posterior Lumbar Interbody Fusion Using Metal Cage
