Radiographic Results of Single Level Transforaminal Lumbar Interbody Fusion in Degenerative Lumbar Spine Disease: Focusing on Changes of Segmental Lordosis in Fusion Segment
- Affiliations
-
- 1Department of Orthopaedic Surgery, Konyang Universitiy College of Medicine, Daejeon, Korea. sirjeon@kyuh.co.kr
- 2Department of Radiology, Konyang Universitiy College of Medicine, Daejeon, Korea.
- KMID: 999403
- DOI: http://doi.org/10.4055/cios.2009.1.4.207
Abstract
- BACKGROUND
To assess the radiographic results in patients who underwent transforaminal lumbar interbody fusion (TLIF), particularly the changes in segmental lordosis in the fusion segment, whole lumbar lordosis and disc height.
METHODS
Twenty six cases of single-level TLIF in degenerative lumbar diseases were analyzed. The changes in segmental lordosis, whole lumbar lordosis, and disc height were evaluated before surgery, after surgery and at the final follow-up.
RESULTS
The segmental lordosis increased significantly after surgery but decreased at the final follow-up. Compared to the preoperative values, the segmental lordosis did not change significantly at the final follow-up. Whole lumbar lordosis at the final follow-up was significantly higher than the preoperative values. The disc height was significantly higher in after surgery than before surgery (p = 0.000) and the disc height alter surgery and at the final follow-up was similar.
CONCLUSIONS
When performing TLIF, careful surgical techniques and attention are needed to restore and maintain the segmental lordosis at the fusion level.
Keyword
MeSH Terms
Figure
-

Fig. 1 The gross morphology of the cage inserted in the procedure.
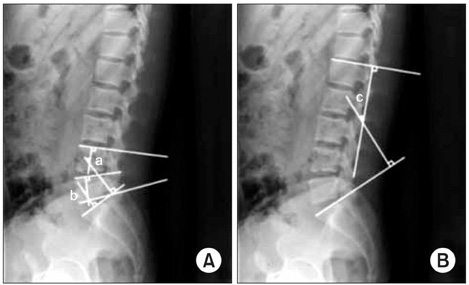
Fig. 2 Cobb's angle for segmental lordosis and whole lumbar lordosis. (A) The segmental lordosis (SL) at L4-5 (a) was defined as the angle subtended by the superior endplate line of L4 and the inferior endplate line of L5. The SL at L5-S1 (b) was defined as the angle subtended by the superior endplate line of L5 and superior endplate line of S1. (B) The whole lumbar lordosis (c) was defined as the angle subtended by the superior endplate line of L1 and superior endplate line of S1.
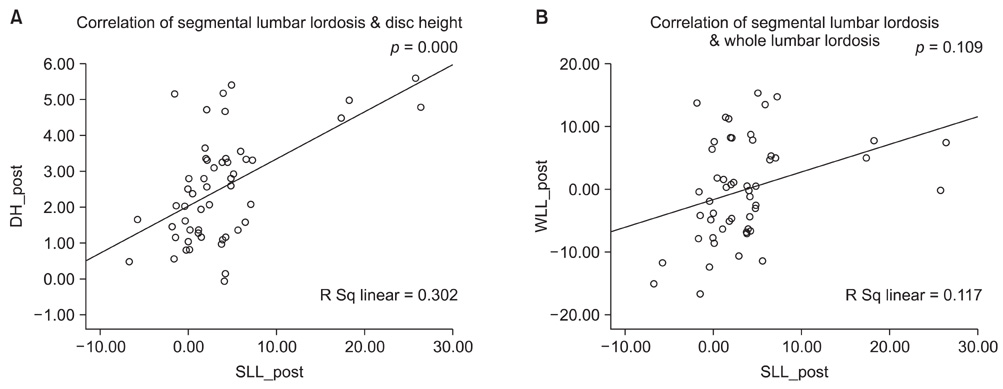
Fig. 3 Correlation between both the segmental lordosis and disc height (A) and segmental lordosis and whole lumbar lordosis (B) after surgery. The graph shows a positive correlation between the segmental lordosis and disc height after surgery. However, there was no correlation between the segmental lordosis and whole lumbar lordosis after surgery.
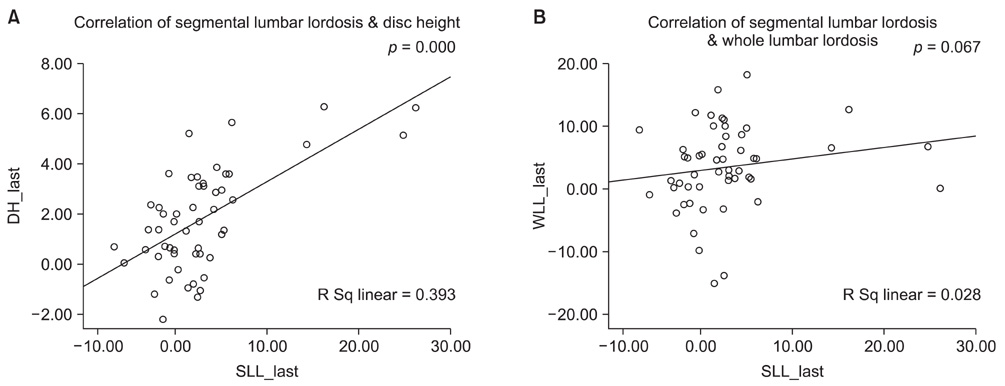
Fig. 4 Correlation between both segmental lordosis and disc height (A) and segmental lordosis and whole lumbar lordosis (B) after the final follow-up. The graph shows a positive correlation between the segmental lordosis and disc height after the last follow-up. However, there was no correlation between the segmental lordosis and whole lumbar lordosis after the last follow up.
Cited by 1 articles
-
Acute Contralateral Radiculopathy after Unilateral Transforaminal Lumbar Interbody Fusion
Kyoung-Min Jang, Seung-Won Park, Young-Baeg Kim, Yong-Sook Park, Taek-Kyun Nam, Young-Seok Lee
J Korean Neurosurg Soc. 2015;58(4):350-356. doi: 10.3340/jkns.2015.58.4.350.
Reference
-
1. Harms JG, Jeszensky D. The unilateral, transforaminal approach for posterior lumbar interbody fusion. Orthop Traumatol. 1998. 6(2):88–99.2. Hee HT, Castro FP Jr, Majd ME, Holt RT, Myers L. Anterior/posterior lumbar fusion versus transforaminal lumbar interbody fusion: analysis of complications and predictive factors. J Spinal Disord. 2001. 14(6):533–540.
Article3. Humphreys SC, Hodges SD, Patwardhan AG, Eck JC, Murphy RB, Covington LA. Comparison of posterior and transforaminal approaches to lumbar interbody fusion. Spine (Phila Pa 1976). 2001. 26(5):567–571.
Article4. Lim HJ, Kwon SC, Roh SW, Jeon SR, Rhim SC. Outcomes of unilateral transforaminal lumbar interbody fusion in degenerative lumbar spine disease. Korean J Spine. 2005. 2(1):19–25.5. Potter BK, Freedman BA, Verwiebe EG, Hall JM, Polly DW Jr, Kuklo TR. Transforaminal lumbar interbody fusion: clinical and radiographic results and complications in 100 consecutive patients. J Spinal Disord Tech. 2005. 18(4):337–346.6. Rosenberg WS, Mummaneni PV. Transforaminal lumbar interbody fusion: technique, complications, and early results. Neurosurgery. 2001. 48(3):569–574.
Article7. Salehi SA, Tawk R, Ganju A, LaMarca F, Liu JC, Ondra SL. Transforaminal lumbar interbody fusion: surgical technique and results in 24 patients. Neurosurgery. 2004. 54(2):368–374.
Article8. Lee SH, Kim YB, Kim TS, et al. Transforaminal lumbar interbody fusion for the treatment of nonunion after posterolateral lumbar fusion. J Korean Soc Spine Surg. 2004. 11(4):223–230.
Article9. Whitecloud TS 3rd, Roesch WW, Ricciardi JE. Transforaminal interbody fusion versus anterior-posterior interbody fusion of the lumbar spine: a financial analysis. J Spinal Disord. 2001. 14(2):100–103.
Article10. Akamaru T, Kawahara N, Tim Yoon S, et al. Adjacent segment motion after a simulated lumbar fusion in different sagittal alignments: a biomechanical analysis. Spine (Phila Pa 1976). 2003. 28(14):1560–1566.
Article11. Brantigan JW, Neidre A. Achievement of normal sagittal plane alignment using a wedged carbon fiber reinforced polymer fusion cage in treatment of spondylolisthesis. Spine J. 2003. 3(3):186–196.
Article12. Diedrich O, Perlick L, Schmitt O, Kraft CN. Radiographic spinal profile changes induced by cage design after posterior lumbar interbody fusion preliminary report of a study with wedged implants. Spine (Phila Pa 1976). 2001. 26(12):E274–E280.13. Lee DY, Lee SH, Lee HS. Transforaminal lumbar interbody fusion using wedged cages for isthmic spondylolisthesis: a short-term radiological analysis. J Korean Neurosurg Soc. 2006. 40(5):346–350.14. Kim EH, Lee JH, Sihn DH, Kim YE, Jae HW. Factors affecting segmental lordotic angle after posterior lumbar interbody fusion using metal cage. J Korean Soc Spine Surg. 2005. 12(4):316–323.
Article15. Godde S, Fritsch E, Dienst M, Kohn D. Influence of cage geometry on sagittal alignment in instrumented post erior lumbar interbody fusion. Spine (Phila Pa 1976). 2003. 28(15):1693–1699.16. Goldstein JA, Macenski MJ, Griffith SL, McAfee PC. Lumbar sagittal alignment after fusion with a threaded interbody cage. Spine (Phila Pa 1976). 2001. 26(10):1137–1142.
Article17. Groth AT, Kuklo TR, Klemme WR, Polly DW, Schroeder TM. Comparison of sagittal contour and posterior disc height following interbody fusion: threaded cylindrical cages versus structural allograft versus vertical cages. J Spinal Disord Tech. 2005. 18(4):332–336.
Article18. Kim JS, Oh SH, Kim SB, Yi HJ, Ko Y, Kim YS. Wedge shape cage in posterior lumbar interbody fusion: focusing on changes of lordotic curve. J Korean Neurosurg Soc. 2005. 38(4):255–258.19. Klemme WR, Owens BD, Dhawan A, Zeidman S, Polly DW Jr. Lumbar sagittal contour after posterior interbody fusion: threaded devices alone versus vertical cages plus posterior instrumentation. Spine (Phila Pa 1976). 2001. 26(5):534–537.20. Umehara S, Zindrick MR, Patwardhan AG, et al. The biomechanical effect of postoperative hypolordosis in instrumented lumbar fusion on instrumented and adjacent spinal segments. Spine (Phila Pa 1976). 2000. 25(13):1617–1624.
Article21. Kwon BK, Berta S, Daffner SD, et al. Radiographic analysis of transforaminal lumbar interbody fusion for the treatment of adult isthmic spondylolisthesis. J Spinal Disord Tech. 2003. 16(5):469–476.
Article22. Schlegel JD, Smith JA, Schleusener RL. Lumbar motion segment pathology adjacent to thoracolumbar, lumbar, and lumbosacral fusions. Spine (Phila Pa 1976). 1996. 21(8):970–981.
Article23. Jackson RP, McManus AC. Radiographic analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex, and size: a prospective controlled clinical study. Spine (Phila Pa 1976). 1994. 19(14):1611–1618.
Article24. Kawakami M, Tamaki T, Ando M, Yamada H, Hashizume H, Yoshida M. Lumbar sagittal balance influences the clinical outcome after decompression and posterolateral spinal fusion for degenerative lumbar spondylolisthesis. Spine (Phila Pa 1976). 2002. 27(1):59–64.
Article25. Oda I, Cunningham BW, Buckley RA, et al. Does spinal kyphotic deformity influence the biomechanical characteristics of the adjacent motion segments An in vivo animal model. Spine (Phila Pa 1976). 1999. 24(20):2139–2146.
Article26. Kim SB, Jeon TS, Ryu SR, Kim SH, Hwang CM. Unilateral transforaminal lumbar interbody fusion in spondylolisthesis: comparison with conventional posterior lumbar interbody fusion through bilateral approach. J Korean Soc Spine Surg. 2008. 15(2):87–95.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Outcomes of Multi-Level Anterior, Oblique, Transforaminal Lumbar Interbody Fusion Surgery : Impact on Global Sagittal Alignment
- Restoration of Lumbar Lordosis After Posterior Lumbar Interbody Fusion with 4 Degree Cage in Degenerative Spinal Disease
- Radiographic Results of Minimally Invasive (MIS) Lumbar Interbody Fusion (LIF) Compared with Conventional Lumbar Interbody Fusion
- Uniportal Endoscopic Lumbar Interbody Fusion
- Restoration of Segmental Lordosis and Related Factors in Interbody Fusion for Degenerative Lumbar Disease
