Factors Affecting Segmental Lordotic Angle After Posterior Lumbar Interbody Fusion Using Metal Cage
- Affiliations
-
- 1Department of Orthopedic Surgery, Soonchunhyang University College of Medicine, Bucheon, Korea.
- 2Department of Orthopedic Surgery, National Medical Center, Seoul, Korea. ljhos@medimail.co.kr
Abstract
- STUDY DESIGN: This is a retrospective study.
OBJECTIVES
We tried to find out what kind of factors affect the segmental lordotic angle improvement after performing posterior lumbar interbody (PLIF) fusion using a metal cage. The study was done using radiographic measurements. SUMMARY OF LITERATURE REVIEW: For degenerative spinal disease, PLIF with using a metal cage is an effective way to fuse and restore segmental lordosis of the lumbar spine.
MATERIALS AND METHODS
The study included 104 patients (65 males, 39 females). Radiographs of the antero-posterior, lateral, flexion and extension views that were taken during the preoperative period and the follow-up 6 months were evaluated for the L4-5 segmental lordosis angle, cage invagination, cage position and disc height. Then, statistical analysis was performed using the Pearson method to determine which factors affected the segmental lordotic angle correction.
RESULTS
The increase of the anterior disc height on the postoperative lateral radiograph (gamma=0.303, p<0.01) and the increase of lordosis on the preoperative extension radiograph (gamma=0.384, p<0.01) showed statistically positive correlation with the increase of the postoperative segmental lordosis angle. When comparing between the 4 degrees and 8 degrees cages, the more angle the cage had, the more segmental angle was restored and this was statistically correlated (P<0.05). However, the amount of segmental lordosis angle correction was not as much as the angle of the cage that was used. Other factors such as cage invagination and cage position didn't show statistical correlation.
CONCLUSIONS
Posterior lumbar interbody fusion using a metal cage is useful method for restoring the lumbar segmental lordosis angle only if the disc is flexible enough to be distracted (ED note: distracted is the word you want?) sufficiently intraoperatively or if it allows good segmental lordosis, as seen on the preoperative extension radiograph. Correction of the segmental lordosis angle using a wedged cage with a larger angle was not always satisfactory because it did not restore as much angle as the angle of cage that was used.
MeSH Terms
Figure
-
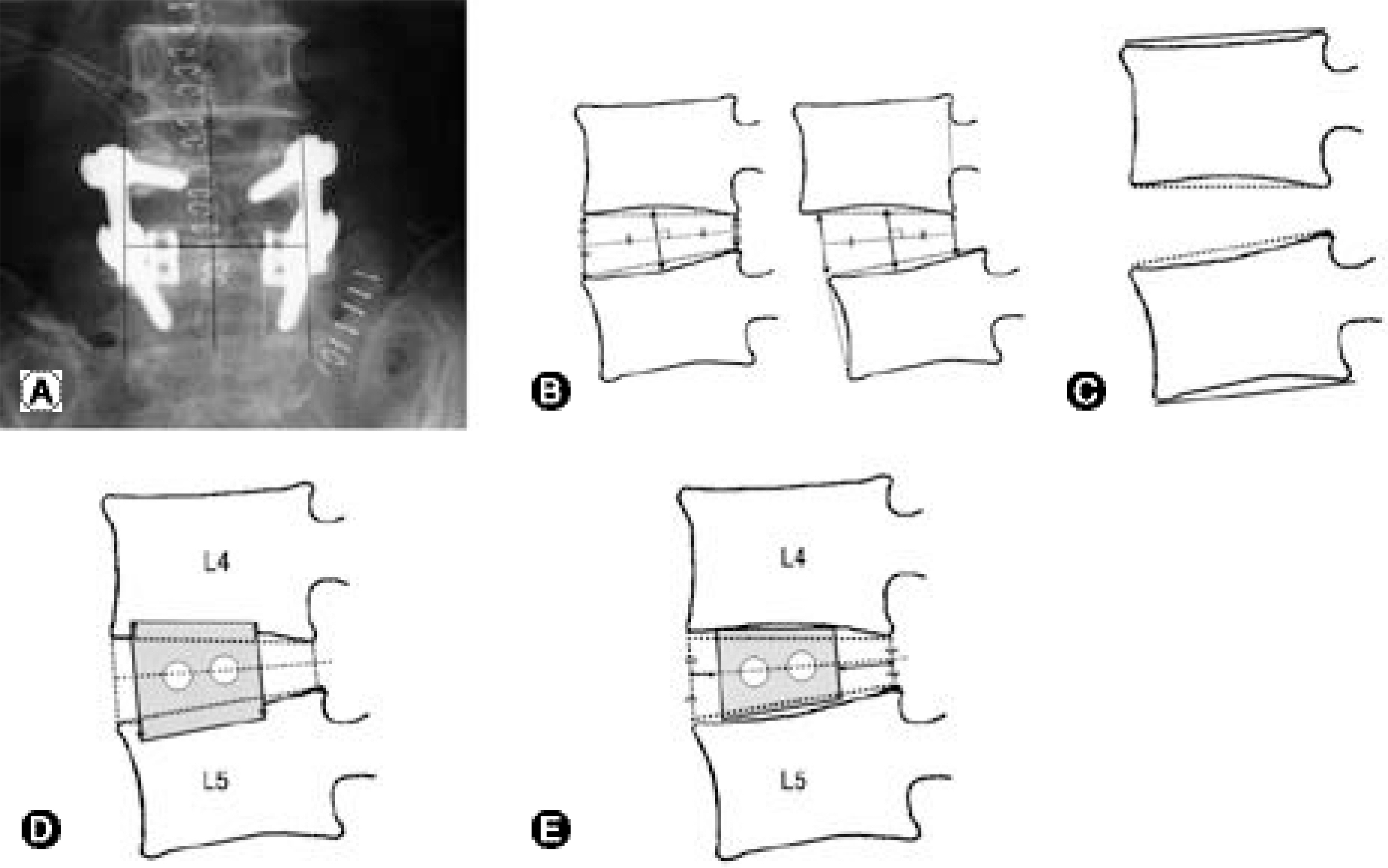
Fig. 1. (A) Cage position on coronal plane was measured by distance of medial margin of each cage from spinous process. (B) Disc space height was measured from anterior, middle and posterior margin of disc. (C). Segmental lordosis angle of L4-5 was measured from cobb's angle beetween upper and lower end plate. (D) Cage invagination was measured from 4 position. Anterior-superior, anterior-inferior, posterior-superior, posterior-inferior. (E) Cage position was measured in lateral film by the distance from anterior disc margin to anterior margin of cage and posterior disc margin to posterior margin of cage.
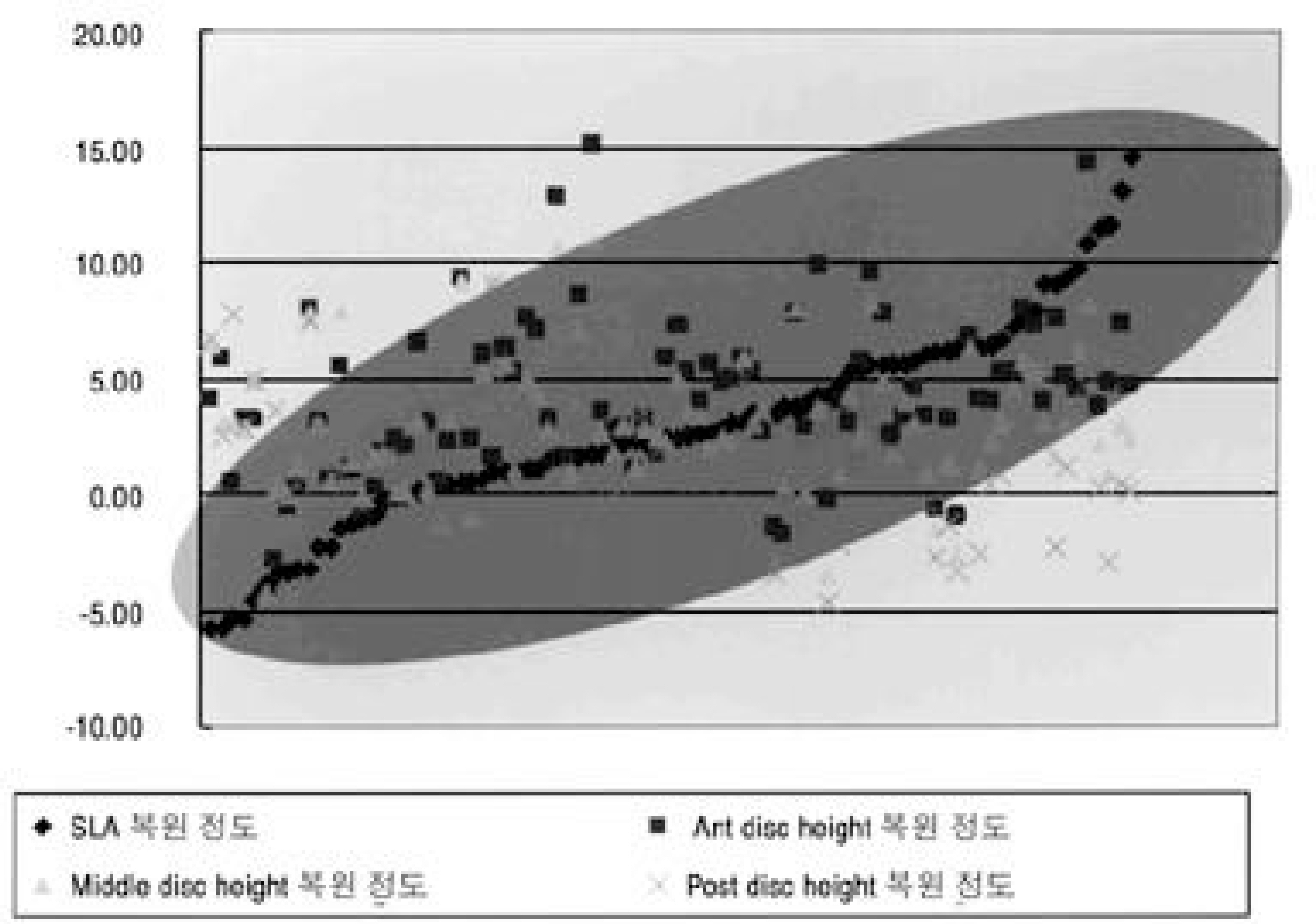
Fig. 2. The more anterior disc height was restored postoperatively, the more segmental lordosis angle was restored.
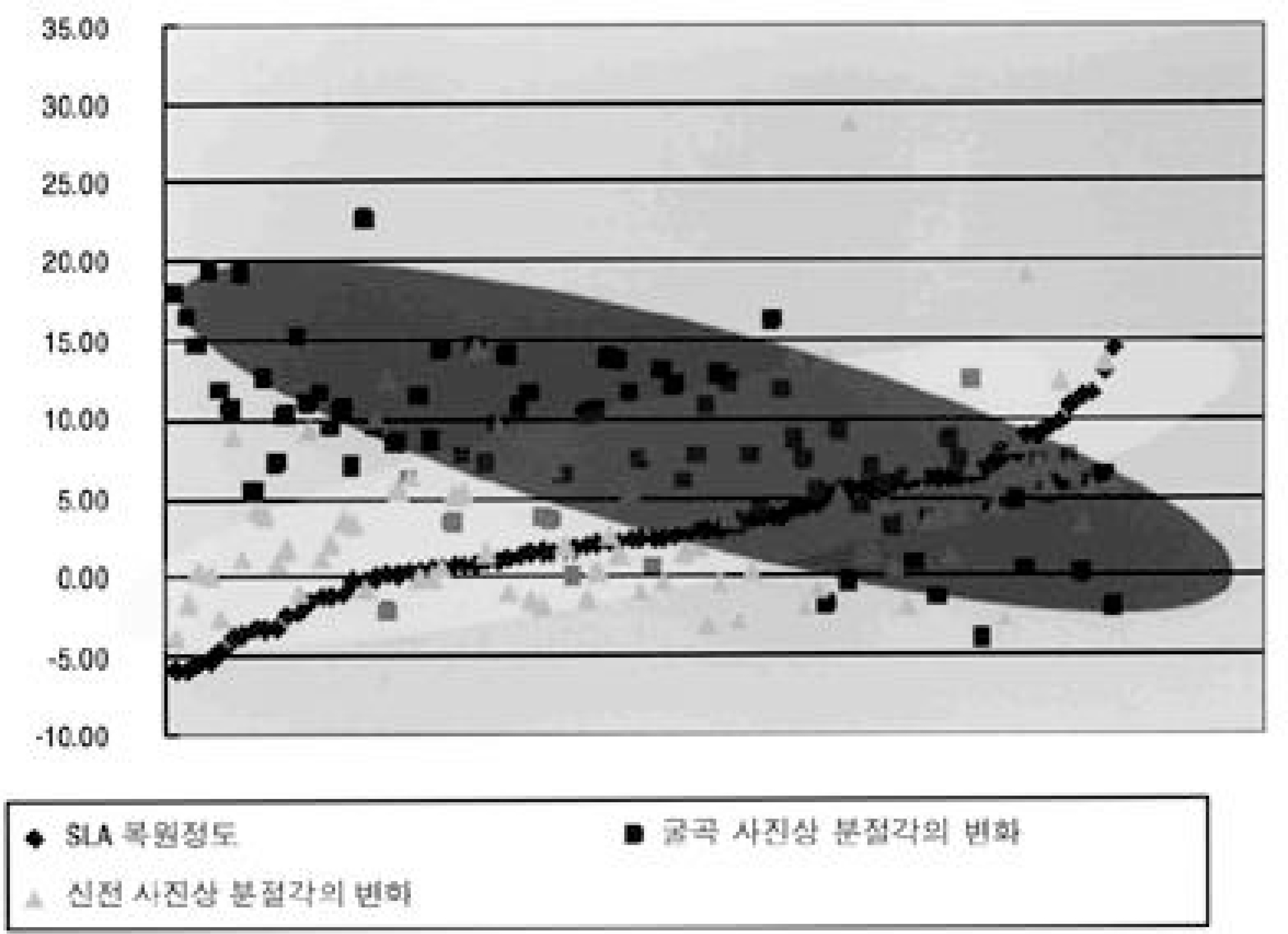
Fig. 3. The more lordotic change was noted on preoperative extension view, the more segmetal lordotic angle was restored, the less kyphotic change was noted on preoperative flexion view, the more segmental lordotic angle was resoted.
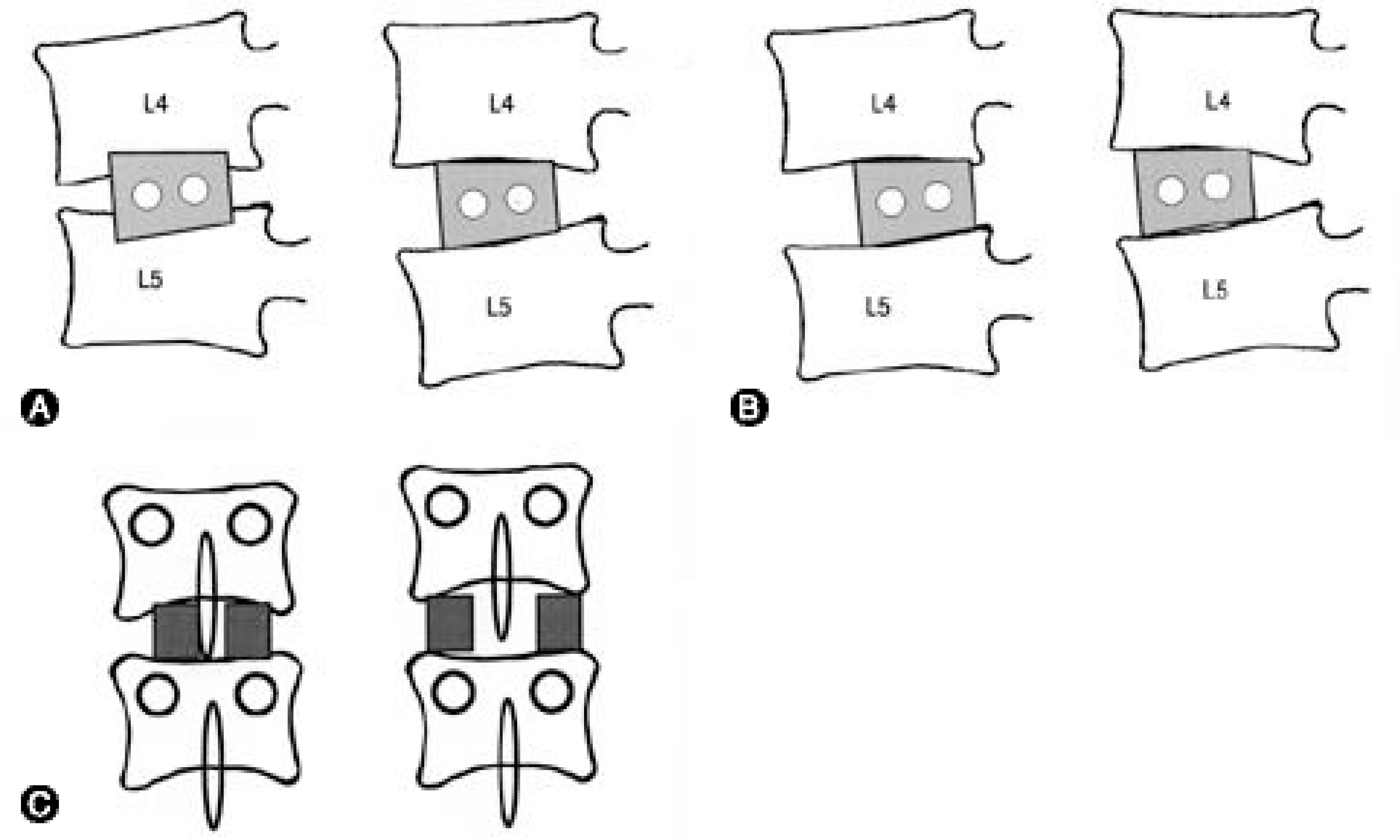
Fig. 4. (A) The cage invagination into end plate would decrease the amount of segmental lordosis angle restoration. (B) The more cage advancement into anterior, the more segmental lordosis angle will be restored. (C). On coronal plane, the more cage divergence, the more intervertebral disc space widening will happen.
Reference
-
1). Abumi K, Panjabi MM, Kramer KM, Duranceau J, Oxland T, Crisco JJ. Biomechanical evaluation of lumbar spinal stability after graded facetectomies. Spine. 1990; 15:1142–1147.
Article2). Beckers L, Bekaert J. The role of lordosis. Acta Orthop Belg. 1991; 57:198–202.3). Glazer PA, Colliou O, Lotz JC, Bradford DS. Biomechanical analysis of lumbosacral fixation. Spine. 1996; 21:1211–1222.
Article4). Jackson RP, McMagnus AC. Radiographic analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex and size: a prospective controlled clinical study. Spine. 1994; 19:1611–1618.5). Jackson RP, Peterson MD, McMagnus AC, Hales C. Compensatory spinopelvic balance over the hip axis and better reliability in measuring lordosis to the pelvic radius on standing lateral radiographs of adult volunteers and patients. Spine. 1998; 23:1750–1767.
Article6). LaGrone MO, Bradford DS, Moe JH, Lonstein JE, Winter RB. Treatment of symptomatic flatback after spinal fusion. J Bone Joint Surg Am. 1988; 70:569–580.
Article7). Lund T, Oxland TR, Jost B, et al. Interbody cage stabil -isation in the lumbar spine: biomechanical evaluation of cage design, posterior instrumentation and bone density. J Bone Joint Surg Br. 1998; 80:351–359.8). Rapoff JA, Ghanayem AJ, Zdeblick TA. Biomechanical comparison of posterior lumbar interbody fusion cages. Spine. 1997; 22:2375–2379.
Article9). Tribus CB, Belanger TA, Zdeblick TA. The effect of operative position and short-segment fusion on maintenance of sagittal alignment of the lumbar spine. Spine. 1999; 24:58–61.
Article10). Diedrich O, Perlick L, Schmitt O, Kraft CN. Rad i -ographic spinal profile changes induced by cage design after posterior lumbar interbody fusion. Preliminary report of a study with wedged implants. Spine. 2001; 26:E274–280.11). Kuslich SD, Ulstrom CL, Griffith SL, Ahern JW, Dow-dle JD. The Bagdy and Kuslich method of lumbar interbody fusion: history, techniques, and 2-year follow-up results of a United States prospective, multicenter trial. Spine. 1998; 23:1267–1279.12). Thomson JD, Renshaw TS. Analysis of lumbar lordosis in posterior spine fusion for idiopathic scoliosis. J Spinal Disord. 1989; 2:93–98.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Wedge Shape Cage in Posterior Lumbar Interbody Fusion: Focusing on Changes of Lordotic Curve
- Restoration of Segmental Lordosis and Related Factors in Interbody Fusion for Degenerative Lumbar Disease
- Lumbar Lordosis Restoration with an Eight Degree Cage in Posterior Lumbar Interbody Fusion for Lumbar Degenerative Disease
- Restoration of Lumbar Lordosis After Posterior Lumbar Interbody Fusion with 4 Degree Cage in Degenerative Spinal Disease
- Prognostic Factors of the Posterior Lumbar Interbody Fusion with Expandable Cage
