Yonsei Med J.
2015 Mar;56(2):582-585. 10.3349/ymj.2015.56.2.582.
Rifampicin-Induced Minimal Change Disease Is Improved after Cessation of Rifampicin without Steroid Therapy
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. ohjmd@yuhs.ac
- 2Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2070042
- DOI: http://doi.org/10.3349/ymj.2015.56.2.582
Abstract
- There are several reports to demonstrate that rifampicin, a major anti-tuberculosis agent, is associated with some adverse renal effects, with a few cases of rifampicin-induced minimal change disease (MCD). In the present case, a 68-year-old female presented with nausea, vomiting, foamy urine, general weakness and edema. She had been taking rifampicin for 4 weeks due to pleural tuberculosis. The patient had no proteinuria before the anti-tuberculosis agents were started, but urine tests upon admission showed heavy proteinuria with a 24-h urinary protein of 9.2 g/day, and serum creatinine, albumin, and total cholesterol levels were 1.36 mg/dL, 2.40 g/dL, and 283 mg/dL, respectively. MCD was diagnosed, and the patient achieved complete remission after cessation of rifampicin without undergoing steroid therapy.
Keyword
MeSH Terms
-
Aged
Antibiotics, Antitubercular/*adverse effects/therapeutic use
Edema/etiology
Female
Humans
Kidney Function Tests
Kidney Glomerulus/pathology
Nausea/etiology
Nephrosis, Lipoid/*chemically induced/pathology
Proteinuria
Remission Induction
Rifampin/*adverse effects/therapeutic use
Treatment Outcome
Tuberculosis, Pleural/*drug therapy
Antibiotics, Antitubercular
Rifampin
Figure
-

Fig. 1 (A) Light microscopy shows minor abnormalities of the glomeruli. The tubules show minimal atrophy and mild focal tubular injury. The interstitium is widened by minimal fibrosis. Non-sclerotic glomeruli are normocellular without mesangial expansion (H&E staining). (B) Electron microscopy shows diffusely effaced foot processes. The glomerular basement membranes are relatively even, but focal thinning of the lamina densa is noted. The mesangium is not expanded and is free of electron-dense deposits (H&E staining).
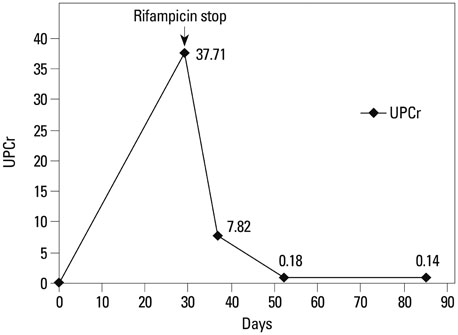
Fig. 2 Clinical course. After discontinuation of rifampicin, the UPCr was recovered. UPCr, random urine protein-to-creatinine ratio.
Reference
-
1. Covic A, Goldsmith DJ, Segall L, Stoicescu C, Lungu S, Volovat C, et al. Rifampicin-induced acute renal failure: a series of 60 patients. Nephrol Dial Transplant. 1998; 13:924–929.
Article2. De Vriese AS, Robbrecht DL, Vanholder RC, Vogelaers DP, Lameire NH. Rifampicin-associated acute renal failure: pathophysiologic, immunologic, and clinical features. Am J Kidney Dis. 1998; 31:108–115.
Article3. Gabow PA, Lacher JW, Neff TA. Tubulointerstitial and glomerular nephritis associated with rifampin. Report of a case. JAMA. 1976; 235:2517–2518.
Article4. Kohno K, Mizuta Y, Yoshida T, Watanabe H, Nishida H, Fukami K, et al. Minimal change nephrotic syndrome associated with rifampicin treatment. Nephrol Dial Transplant. 2000; 15:1056–1059.
Article5. Murray AN, Cassidy MJ, Templecamp C. Rapidly progressive glomerulonephritis associated with rifampicin therapy for pulmonary tuberculosis. Nephron. 1987; 46:373–376.
Article6. Muthukumar T, Jayakumar M, Fernando EM, Muthusethupathi MA. Acute renal failure due to rifampicin: a study of 25 patients. Am J Kidney Dis. 2002; 40:690–696.
Article7. Neugarten J, Gallo GR, Baldwin DS. Rifampin-induced nephrotic syndrome and acute interstitial nephritis. Am J Nephrol. 1983; 3:38–42.
Article8. Rekha VV, Santha T, Jawahar MS. Rifampicin-induced renal toxicity during retreatment of patients with pulmonary tuberculosis. J Assoc Physicians India. 2005; 53:811–813.9. Tada T, Ohara A, Nagai Y, Otani M, Ger YC, Kawamura S. A case report of nephrotic syndrome associated with rifampicin therapy. Nihon Jinzo Gakkai Shi. 1995; 37:145–150.10. Yoshioka K, Satake N, Kasamatsu Y, Nakamura Y, Shikata N. Rapidly progressive glomerulonephritis due to rifampicin therapy. Nephron. 2002; 90:116–118.
Article11. Black DA, Rose G, Brewer DB. Controlled trial of prednisone in adult patients with the nephrotic syndrome. Br Med J. 1970; 3:421–426.
Article12. Waldman M, Crew RJ, Valeri A, Busch J, Stokes B, Markowitz G, et al. Adult minimal-change disease: clinical characteristics, treatment, and outcomes. Clin J Am Soc Nephrol. 2007; 2:445–453.
Article13. Glassock RJ. Secondary minimal change disease. Nephrol Dial Transplant. 2003; 18:Suppl 6. vi52–vi58.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rifampicin-Induced Severe Hyperkalemia Requiring Hemodialysis in a Patient with Addison's Disease
- A Case of Rifampicin-induced Thrombocytopenic Purpura
- Tracing the Variation in Physiological Response to Rifampicin Across the Microbial Spectrum
- Rifampicin Inhibits the LPS-induced Expression of Toll-like Receptor 2 via the Suppression of NF-kappaB DNA-binding Activity in RAW 264.7 Cells
- Rifampicin-induced Tubulo-interstitial Nephritis - A case report -
