Korean Circ J.
2015 Jul;45(4):317-324. 10.4070/kcj.2015.45.4.317.
Cardiac Function in Kawasaki Disease Patients with Respiratory Symptoms
- Affiliations
-
- 1Department of Pediatrics, Ewha Womans University School of Medicine, Seoul, Korea. ymhong@ewha.ac.kr
- KMID: 1964104
- DOI: http://doi.org/10.4070/kcj.2015.45.4.317
Abstract
- BACKGROUND AND OBJECTIVES
Respiratory symptoms are often observed in children with Kawasaki disease (KD) during the acute phase. The association of respiratory viruses in children with KD was investigated using multiplex reverse transcriptase-polymerase chain reaction (RT-PCR) and tissue Doppler echocardiography.
SUBJECTS AND METHODS
138 KD patients were included from January 2010 to June 2013. We compared 3 groups (group 1: n=94, KD without respiratory symptoms; group 2: n=44, KD with respiratory symptoms; and group 3: n=50, febrile patients with respiratory symptoms). Laboratory data were obtained from each patient including N-terminal pro-brain natriuretic peptide (NT-proBNP). Echocardiographic measurements were compared between group 1 and group 2. RT-PCR was performed using nasopharyngeal secretion to screen for the presence of 14 viruses in groups 2 and 3.
RESULTS
The incidence of KD with respiratory symptoms was 31.8%. The duration of fever was significantly longer, and coronary artery diameter was larger in group 2 than in group 1. Tei index was significantly higher and coronary artery diameter larger in group 2 than group 1. Coronary artery diameter, C-reactive protein levels, platelet count, alanine aminotransferase levels, and NT-pro BNP levels were significantly higher and albumin levels lower in group 2 compared with group 3.
CONCLUSION
NT-pro BNP was a valuable diagnostic tool in differentiating KD from other febrile viral respiratory infections. Some viruses were more frequently observed in KD patients than in febrile controls. Tei index using tissue Doppler imaging was increased in KD patients with respiratory symptoms.
Keyword
MeSH Terms
-
Alanine Transaminase
C-Reactive Protein
Child
Coronary Vessels
Echocardiography
Echocardiography, Doppler
Fever
Humans
Incidence
Mucocutaneous Lymph Node Syndrome*
Natriuretic Peptide, Brain
Platelet Count
Respiratory Tract Infections
Reverse Transcriptase Polymerase Chain Reaction
Alanine Transaminase
C-Reactive Protein
Natriuretic Peptide, Brain
Figure
-

Fig. 1 Tei index using tissue Doppler imaging in Kawasaki disease patients. Tei index= (a-b)/b=(IVCT+IVRT)/ET. IVCT: isovolumetric contraction time, IVRT: isovolumetric relaxation time, ET: ejection time, LV Eject T: left ventricular ejection time, S': systolic myocardial velocity, A': late diastolic myocardial velocity, E': early diastolic myocardial velocity.
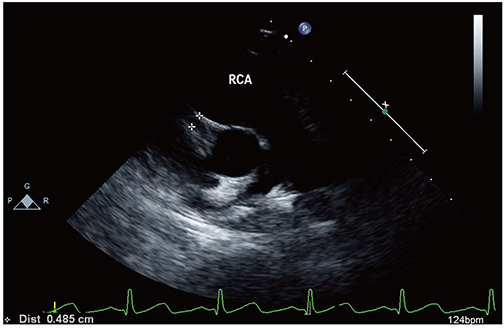
Fig. 2 Parasternal short axis echocardiographic imaging showing a dilated right coronary artery. RCA: right coronary artery.
Cited by 1 articles
-
Comparison of Clinical Manifestation and Laboratory Findings between Adenoviral Infection with or without Kawasaki Disease
Yu Jin Kwak, Yi Kyung Kim, Ji Eun Ban, Sejung Sohn, Young Mi Hong
Ewha Med J. 2018;41(3):45-52. doi: 10.12771/emj.2018.41.3.45.
Reference
-
1. Kawasaki T, Kosaki F, Okawa S, Shigematsu I, Yanagawa H. A new infantile acute febrile mucocutaneous lymph node syndrome (MLNS) prevailing in Japan. Pediatrics. 1974; 54:271–276.2. Burns JC, Glodé MP. Kawasaki syndrome. Lancet. 2004; 364:533–544.3. Wood LE, Tulloh RM. Kawasaki disease in children. Heart. 2009; 95:787–792.4. Kim GB, Park S, Kwon BS, Han JW, Park YW, Hong YM. Evaluation of the temporal association between Kawasaki disease and viral infections in South Korea. Korean Circ J. 2014; 44:250–254.5. Chang LY, Lu CY, Shao PL, et al. Viral infections associated with Kawasaki disease. J Formos Med Assoc. 2014; 113:148–154.6. Rowley AH, Shulman ST. Kawasaki syndrome. Pediatr Clin North Am. 1999; 46:313–329.7. Yanagawa H, Nakamura Y, Yashiro M, et al. Results of the nationwide epidemiologic survey of Kawasaki disease in 1995 and 1996 in Japan. Pediatrics. 1998; 102:e65.8. Green MS. The male predominance in the incidence of infectious disease in children: a postulated explanation for disparities in the literature. Int J Epidemiol. 1992; 21:381–386.9. Brogan PA, Bose A, Burgner D, et al. Kawasaki disease: an evidence based approach to diagnosis, treatment, and proposals for future research. Arch Dis Child. 2002; 86:286–290.10. Jaggi P, Kajon AE, Mejias A, Ramilo O, Leber A. Human adenovirus infection in Kawasaki disease: a confounding bystander? Clin Infect Dis. 2013; 56:58–64.11. Treadwell TA, Maddox RA, Holman RC, et al. Investigation of Kawasaki syndrome risk factors in Colorado. Pediatr Infect Dis J. 2002; 21:976–978.12. Jordan-Villegas A, Chang ML, Ramilo O, Mejias A. Concomitant respiratory viral infections in children with Kawasaki disease. Pediatr Infect Dis J. 2010; 29:770–772.13. Kim JH, Yu JJ, Lee J, et al. Detection rate and clinical impact of respiratory viruses in children with Kawasaki disease. Korean J Pediatr. 2012; 55:470–473.14. Sanchez Mejia AA, Simpson KE, Hildebolt CF, et al. Tissue Doppler septal Tei index indicates severity of illness in pediatric patients with congestive heart failure. Pediatr Cardiol. 2014; 35:411–418.15. Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the committee on rheumatic fever, endocarditis, and Kawasaki disease, council on cardiovascular disease in the young, American Heart Association. Pediatrics. 2004; 114:1708–1733.16. Park YW, Han JW, Hong YM, et al. Epidemiological features of Kawasaki disease in Korea, 2006-2008. Pediatr Int. 2011; 53:36–39.17. Melish ME. Kawasaki syndrome. Pediatr Rev. 1996; 17:153–162.18. Burns JC, Herzog L, Fabri O, et al. Seasonality of Kawasaki disease: a global perspective. PLoS One. 2013; 8:e74529.19. Tsai HC, Chang LY, Lu CY, et al. Transmission of acute infectious illness among cases of Kawasaki disease and their household members. J Formos Med Assoc. 2015; 114:72–76.20. Principi N, Rigante D, Esposito S. The role of infection in Kawasaki syndrome. J Infect. 2013; 67:1–10.21. Burgner D, Harnden A. Kawasaki disease: what is the epidemiology telling us about the etiology? Int J Infect Dis. 2005; 9:185–194.22. Chang LY, Chang IS, Lu CY, et al. Epidemiological features of Kawasaki disease in Taiwan, 1996-2002. Pediatrics. 2004; 114:e678–e682.23. Nakamura Y, Yanagawa I, Kawasaki T. Temporal and geographical clustering of Kawasaki disease in Japan. Prog Clin Biol Res. 1987; 250:19–32.24. Ye Q, Shao WX, Shang SQ, Zhou MM. Value of the N-terminal of prohormone brain natriuretic peptide in diagnosis of Kawasaki disease. Int J Cardiol. 2015; 178:5–7.25. Dahdah N, Siles A, Fournier A, et al. Natriuretic peptide as an adjunctive diagnostic test in the acute phase of Kawasaki disease. Pediatr Cardiol. 2009; 30:810–817.26. Bae HK, Lee DK, Kwon JH, Kim HS, Sohn S, Hong YM. Clinical characteristics and serum N-terminal pro-brain natriuretic peptide as a diagnostic marker of Kawasaki disease in infants younger than 3 months of age. Korean J Pediatr. 2014; 57:357–362.27. Vijayan AP, Dinesh KB, Nath KR. Coronary artery dilatation in incomplete Kawasaki disease. Indian Pediatr. 2009; 46:607–609.28. Bruch C, Schmermund A, Marin D, et al. Tei-index in patients with mild-to-moderate congestive heart failure. Eur Heart J. 2000; 21:1888–1895.29. Tei C, Dujardin KS, Hodge DO, et al. Doppler echocardiographic index for assessment of global right ventricular function. J Am Soc Echocardiogr. 1996; 9:838–847.30. Ajami G, Borzouee M, Amoozgar H, et al. Evaluation of myocardial function using the Tei index in patients with Kawasaki disease. Cardiol Young. 2010; 20:44–48.
