J Korean Med Assoc.
2005 Sep;48(9):857-868. 10.5124/jkma.2005.48.9.857.
Exercise in the Elderly
- Affiliations
-
- 1Department of Rehabilitation Medicine, Soonchunhyang University College of Medicine and Hospital, Korea. lyg777@hosp.sch.ac.kr
- KMID: 1958310
- DOI: http://doi.org/10.5124/jkma.2005.48.9.857
Abstract
- The health benefits from exercise, particularly in a sedentary society, have gained a compelling body of evidence in the past decade. Younger adults have a considerably bigger physiologic reserve, both in terms of muscular strength and cardiovascular capacity. The elderly, on the other hand, experience a progressive decline in many physiologic functions, including muscular strength and cardiovascular capacity. Habitual exercise, by improving strength and maximum aerobic capacity (VO2max), can increase the physiologic reserve as well as enhance well-being by reducing fatigue associated with activities of daily living. Mostly importantly, it can delay the development of disability and thereby prolong active life expectancy. In addition to habitual exercise for conditioning, there is increasing evidence that resistance exercise to improve muscle strength along with tailored exercise therapies, including those designed to improve balance or to rehabilitate persons with various chronic diseases and acute ailments, may be of special value for the elderly. There is growing evidence that exercise programs offer measurable health benefits, ranging from increased life expectancy to mitigation of adverse sequelae from aging and from many chronic diseases. The greatest challenges in achieving health benefits from exercise are the limited access to effective programs and poor compliance.
Keyword
MeSH Terms
Figure
-

Figure 1 TLC = total lung capacity, FRC = functional residual capacity, RV = residual volume
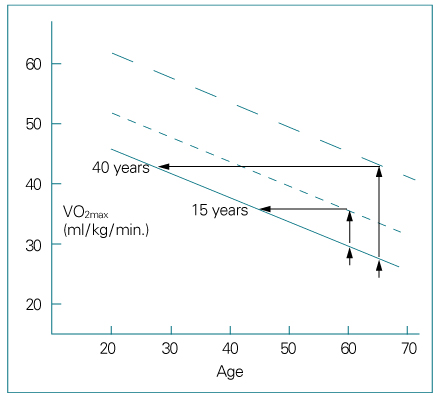
Figure 2
Reference
-
5. Abrass IB. The biology and physiology of aging. West L Med. 1990. 153:641–645.6. Braddom RA. Felsenthal G, Stein BD, editors. Principles of geriatric rehabilitation. Physical medicine & rehabilitation. 1996. Philadelphia: WB Saunders;1242.7. Cassel CK, Leipzig RM, Cohen HJ, Larson EB, Meier DE. Larson EB, Bruce RA, editors. Exercis. Geriatric medicine. 2003. 4th ed. New York: Springer-Verlag;1023–1029.8. Delisa JA. Clark GS, Siebens HC, editors. Rehabilitation of the geriatric patient. Rehabilitation medicine. Principles and Practice. 1993. 2nd ed. Philadelphia: Lippincott;642–665.9. Kawas CH. Felsenthal G, Garrison SJ, Steinberg FU, editors. Evaluation of cognition in the elderly rehabilitation patient. Rehabilitation of Aging and Elderly Patient. 1994. Baltimore: Williams & Wilkins;215–226.10. Geokas MC, Lakatta EG, Makinodan T, Timiras PS. The aging process. Ann Intern Med. 1990. 113:455–466.
Article11. Larson EB, Bruce RA. Health benefits of exercise in aging society. Arch Intern Med. 1987. 147:353–356.12. Mosby's medical, nursing, and allied health dictionary. 1994. 4th ed. St. Louis: Mosby;583–584.13. Naughton J. Physical activity and aging. Prime care. 1982. 9:231–238.
Article14. Poster JD, Gorman KM, Klein HS, Woldow A. Exercise capacity in the elderly. Am J Cardiol. 1986. 57:52C–58C.15. Stern N, Tuck ML. Geriatric cardiology: Homeostatic fragility in the elderly. Cardiol Clin. 1986. 4:201–211.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Individualized Exercise Recommendations for the Frailty Populations: Focusing on Elderly and Cancer Survivors
- Effect of Exercise Program on Physical Strength and Function in Elderly
- Exercise Rehabilitation for Frail Elderly
- Effective Approach to Improving Cognitive Function in the Elderly: Focused on Cognitive-exercise Combination Program
- The Effect of Exercise Program on Health and Depression in the Elderly
