A Case of Wegener's Granulomatosis that Presented as a Single Lung Mass
- Affiliations
-
- 1Department of Internal Medicine, Chonnam National University, Medical School, Gwangju, Korea. cyberkks@chonnam.ac.kr
- KMID: 1877323
- DOI: http://doi.org/10.4046/trd.2007.63.1.88
Abstract
- Wegener's granulomatosis is a disease with an unknown etiology that is characterized by necrotizing granulomatous vasculitis involving the upper and lower respiratory tract and the kidneys. The typical pulmonary findings are bilaterally involved multiple variable sized nodules. We report a case of Wegener's granulomatosis that presented as a single lung mass. A male patient presented with a nasal obstruction, arthralgia, cough, and intermittent dyspnea. The chest radiograph showed a mass, approximately 4.5 cm in diameter, in the right lower lobe. Lung cancer or tuberculosis was initially considered. However, the clinical, laboratory and pathological findings of the mass indicated Wegener's granulomatosis. The patient was administered prednisolone and cyclophosphamide, and improved temporarily. Unfortunately, the immunocompromised patient expired as a result of respiratory failure with pneumonia.
MeSH Terms
Figure
-

Figure 1 (A) An initial chest X-ray showed a soft tissue mass, approximately 4.5 cm in diameter, in the right lower lung field. (B) Water's view showed mucosal thickening of both maxillary sinuses.
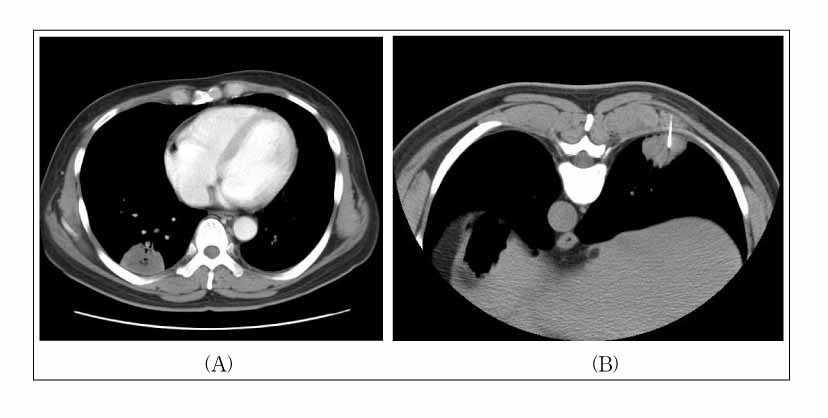
Figure 2 (A) The chest CT showed a 4.5cm-sized nodular lesion in the posterobasal segment of the right lower lobe. (B) A CT-guided transthoracic core needle biopsy for that nodule was performed in the prone position.

Figure 3 Multiple, variable sized purpuras were developed on both lower legs and both feet.
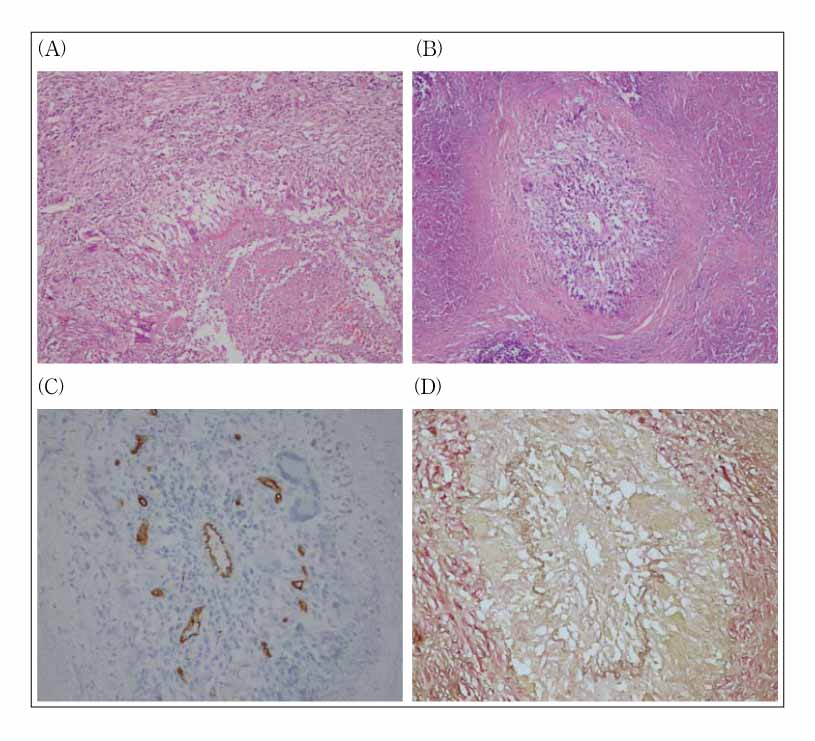
Figure 4 The microscopic findings of the resected pulmonary mass showed (A) a granuloma and (B) necrotizing vasculitis (H&E stain, ×100). These inflammatory lesions were positive in immunohistochemical stains for (C) CD 34 and (D) elastin (immunohistochemical stain, ×200).
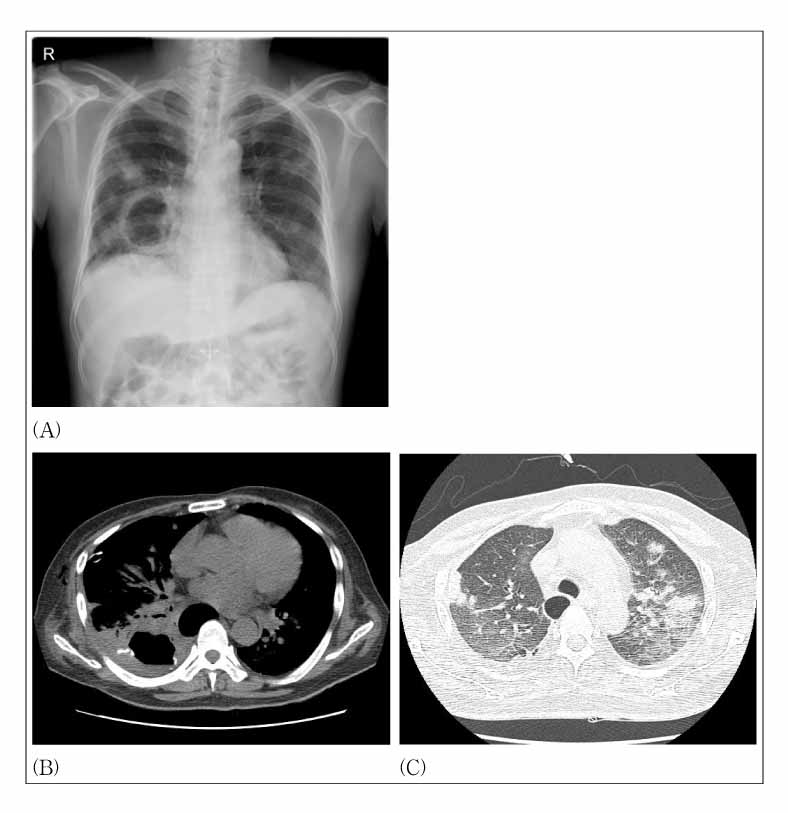
Figure 5 (A) A follow up chest X-ray showed increased size of the cavitary lesion in the right lower lung, with multifocal ill-defined opacities in both lungs. The chest CT showed (B) markedly increased size of the previously noted irregular cavitary mass in the right lower lobe and (C) increased sizes and numbers of multiple nodules with ground glass opacity halos in both upper lobes.
Reference
-
1. Hoffman GS, Kerr GS, Leavitt RY, Hallahan CW, Lebovics RS, Travis WD, et al. Wegener's granulomatosis: an analysis of 158 patients. Ann Intern Med. 1992. 116:488–498.2. Nishino H, DeRemee RA, Rubino FA, Parisi JE. Wegener's granulomatosis associated with vasculitis of the temporal artery: report of five cases. Mayo Clin Proc. 1993. 68:115–121.3. Cordier JF, Valeyre D, Guillevin L, Loire R, Brechot JM. Pulmonary Wegener's granulomatosis. A clinical and imaging study of 77 cases. Chest. 1990. 97:906–912.4. Maguire R, Fauci AS, Doppman JL, Wolff SM. Unusual radiographic features of Wegener's granulomatosis. Am J Roentgenol. 1978. 130:233–238.5. Aberle DR, Gamsu G, Lynch D. Thoracic manifestations of Wegener granulomatosis: diagnosis and course. Radiology. 1990. 174:703–709.6. Rao JK, Weinberger M, Oddone EZ, Allen NB, Landsman P, Feussner JR. The role of antineutrophil cytoplasmic antibody (c-ANCA) testing in the diagnosis of Wegener granulomatosis. A literature review and meta-analysis. Ann Intern Med. 1995. 123:925–932.7. Niles JL, Pan GL, Collins AB, Shannon T, Skates S, Fienberg R, et al. Antigen-specific radioimmunoassays for anti-neutrophil cytoplasmic antibodies in the diagnosis of rapidly progressive glomerulonephritis. J Am Soc Nephrol. 1991. 2:27–36.8. Kallenberg CG, Brouwer E, Weening JJ, Tervaert JW. Anti-neutrophil cytoplasmic antibodies: current diagnostic and pathophysiological potential. Kidney Int. 1994. 46:1–15.9. Weber MF, Andrassy K, Pullig O, Koderisch J, Netzer K. Antineutrophil-cytoplasmic antibodies and antiglomerular basement membrane antibodies in Goodpasture's syndrome and in Wegener's granulomatosis. J Am Soc Nephrol. 1992. 2:1227–1234.10. Specks U, DeRemee RA. Granulomatous vasculitis. Wegener's granulomatosis and Churg-Strauss syndrome. Rheum Dis Clin North Am. 1990. 16:377–397.11. Stokes TC, McCann BG, Rees RT, Sims EH, Harrison BD. Acute fulminating intrapulmonary hemorrhage in Wegener's granulomatosis. Thorax. 1982. 37:315–316.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fine Needle Aspiration Cytology of Pulmonary Lesions in Wegener's Granulomatosis: A Case Report
- A case of Wegener's granulomatosis complicated by non-small cell lung cancer
- A Case of Cortical Vein Thrombosis in Wegener's Granulomatosis
- Localized Wegener's Granulomatosis in Maxillary Sinus
- A case of Wegener's granulomatosis masquerading as a lung abscess
