A Case of Non-Specific Interstitial Pneumonia Associated with Primary Lung Adenocarcinoma
- Affiliations
-
- 1Department of Internal Medicine, Ewha Womans University School of Medicine, Seoul, Korea. jinhwalee@ewha.ac.kr
- 2Department of Radiology, Ewha Womans University School of Medicine, Seoul, Korea.
- 3Department of Pathology, Ewha Womans University School of Medicine, Seoul, Korea.
- 4Department of Thoracic Surgery, Ewha Womans University School of Medicine, Seoul, Korea.
- KMID: 1877322
- DOI: http://doi.org/10.4046/trd.2007.63.1.83
Abstract
- Idiopathic pulmonary fibrosis (IPF) is strongly associated with lung cancer compared with the general population. However, other types of idiopathic interstitial pneumonia (IIP) are rarely associated with lung cancer. We describe a case of a primary lung cancer associated with IIP other than IPF, which was considered to be nonspecific interstitial pneumonia (NSIP), and NSIP disappeared spontaneously after treating the primary lung cancer.
MeSH Terms
Figure
-

Figure 1 A 3-cm sized mass in the left lower lobe.
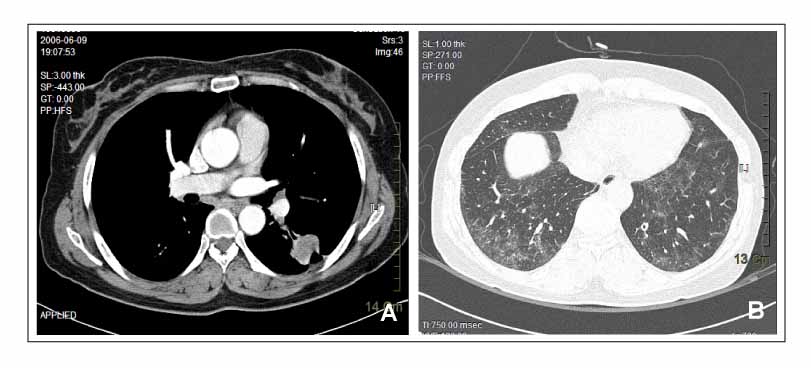
Figure 2 (A) A 3-cm enhancing mass showing air bronchogram and speculated margin with pleural tag is noted in the superior segment of the left lower lobe. (B) Ill-defined ground-glass opacity is noted in both lower lobes, predominantly in peripheral and basal lungs.
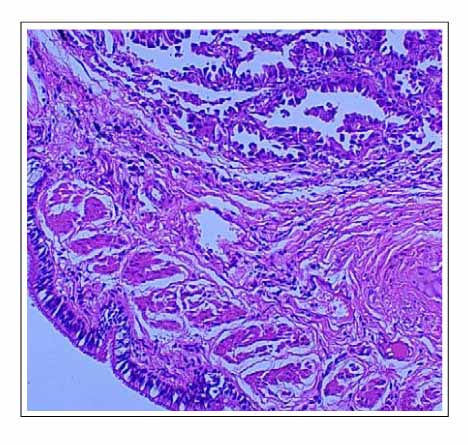
Figure 3 The tumor lesion shows well-to-moderately differentiated neoplastic cells forming acini and tubules composed of cuboid cells, suggesting adenocarcinoma. (H&E stain, ×100)

Figure 4 (A) Non-neoplastic lung parenchyma shows multifocal and diffuse loose interstitial fibrosis with mononuclear infiltration of alveolar walls. The alveolar wall is relatively uniformly thickened. However, the architecture of the lung parenchyma is relatively preserved. (B) Several multinucleated giant cells of undetermined significance, focal collection of desquamated alveolar macrophages with cholesterol clefts are noted. (H&E stain, ×100, A and B)

Figure 5 There is left lower lobectomy state, and previous ground-glass opacity on figure 2B is not noted in the right lower lobe.
Reference
-
1. Matsushita H, Tanaka S, Saiki Y, Hara M, Nakata K, Tanimura S, et al. Lung cancer associated with usual interstitial pneumonia. Pathol Int. 1995. 45:925–932.2. Park J, Kim DS, Shim TS, Lim CM, Koh Y, Lee SD, et al. Lung cancer in patients with idiopathic pulmonary fibrosis. Eur Respir J. 2001. 17:1216–1219.3. Daniels CE, Jett JR. Does interstitial lung disease predispose to lung cancer? Curr Opin Pulm Med. 2005. 11:431–437.4. Yamadori I, Sato T, Fujita J, Dobashi N, Ohtsuki Y, Takahara J. A case of non-specific interstitial pneumonia associated with primary lung cancer: possible role of antibodies to lung cancer cells in the pathogenesis of non-specific interstitial pneumonia. Respir Med. 1999. 93:754–756.5. Sato T, Yamadori I, Fujita J, Hamada N, Yonei T, Bandoh S, et al. Three cases of non-specific interstitial pneumonia associated with primary lung cancer. Intern Med. 2004. 43:721–726.6. Katzenstein AL, Fiorelli RF. Nonspecific interstitial pneumonia/fibrosis. Histologic features and clinical significance. Am J Surg Pathol. 1994. 18:136–147.7. Reyes LJ, Morell F, Xaubet A, Ramirez J, Majo J. Nonspecific interstitial pneumonia: epidemiologic and clinical characteristics. Med Clin. 2006. 126:47–52.8. Patel AM, Davila DG, Peters SG. Paraneoplastic syndromes associated with lung cancer. Mayo Clin Proc. 1993. 68:278–287.9. Bandoh S, Fujita J, Haba R, Tojo Y, Horiike A, Okamoto T, et al. Lung cancer with focal lymphocytic interstitial pneumonia. Intern Med. 2002. 41:997–1001.10. Takanami I, Takeuchi K, Giga M. The prognostic value of natural killer cell infiltration in resected pulmonary adenocarcinoma. J Thorac Cardiovasc Surg. 2001. 121:1058–1063.11. Lee TK, Horner RD, Silverman JF, Chen YH, Jenny C, Scarantino CW. Morphometric and morphologic evaluations in stage III non-small cell lung cancers. Prognostic significance of quantitative assessment of infiltrating lymphoid cells. Cancer. 1989. 63:309–316.12. Lipford EH 3rd, Eggleston JC, Lillemoe KD, Sears DL, Moore GW, Baker RR. Prognostic factors in surgically resected limited-stage, nonsmall cell carcinoma of the lung. Am J Surg Pathol. 1984. 8:357–365.13. Brittenden J, Heys SD, Ross J, Eremin O. Natural killer cells and cancer. Cancer. 1996. 77:1226–1243.14. Johnson SK, Kerr KM, Chapman AD, Kennedy MM, King G, Cockburn JS, et al. Immune cell infiltrates and prognosis in primary carcinoma of the lung. Lung Cancer. 2000. 27:27–35.15. Watanabe S, Sato Y, Kodama T, Shimosato Y. Immunohistochemical study with monoclonal antibodies on immune response in human lung cancers. Cancer Res. 1983. 43:5883–5889.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Idiopathic Interstitial Pneumonias: Radiologic Findings
- Micropapillary Lung Adenocarcinoma with Aerogenous Spread
- A Case of Nonspecific Interstitial Pneumonia with Clinical Course of Rapid Aggravation
- Reported Lung Adenocarcinoma with Idiopathic Pulmonary Fibrosis after Open Lung Biopsy
- Idiopathic interstitial pneumonias: clinical findings, pathogenesis, pathology and radiologic findings
