Definitive extended field intensity-modulated radiotherapy and concurrent cisplatin chemosensitization in the treatment of IB2-IIIB cervical cancer
- Affiliations
-
- 1Department of Radiation Oncology, Qilu Hospital of Shandong University, Jinan, China. qiluchengyf@aliyun.com
- 2Department of Geriatrics, Qilu Hospital of Shandong University, Jinan, China.
- 3Department of Obstetrics and Gynecology, Qilu Hospital of Shandong University, Jinan, China.
- KMID: 1811183
- DOI: http://doi.org/10.3802/jgo.2014.25.1.14
Abstract
OBJECTIVE
To assess the toxicity of delivering extended field intensity-modulated radiotherapy (EF-IMRT) and concurrent cisplatin chemotherapy for locally advanced cervical carcinoma.
METHODS
Forty-five patients who underwent EF-IMRT and concurrent cisplatin chemotherapy for the treatment of stage IB2 to IIIB cervical cancer were retrospectively reviewed. The clinical target volume included all areas of gross and potentially microscopic disease and regional lymph node regions. All patients underwent high-dose-rate brachytherapy. The acute and late toxicity were scored using the Common Terminology Criteria for Adverse Events and the Radiation Therapy Oncology Group late radiation morbidity scoring criteria, respectively.
RESULTS
The median follow-up was 28 months (range, 5 to 62 months). Forty-two patients had a complete response, and three had a persistent disease. Of those 42 patients, 15 patients (35.7%) had recurrence. The regions of recurrence were in-field in 2 patients and out-field in 13 patients. Acute grade > or =3 gastrointestinal, genitourinary and hematologic toxicity occurred in 3, 1, and 9 patients, respectively. Three patients (6.7%) suffered from late grade 3 toxicities. Seven patients experienced ovarian transposition, 5 of those patients (71%) maintained ovarian function. Thirty-eight patients (84.4%) were alive at the last follow-up.
CONCLUSION
Concurrent cisplatin chemotherapy with EF-IMRT was safe. The acute and late toxicities are acceptable. EF-IMRT provides an opportunity to preserve endocrine function for patients with ovarian transposition.
MeSH Terms
Figure
-

Fig. 1 The transverse image of the target volume. (A-C) showing primary tumor and pelvic lymph nodes planning target volume (PTV) depicted in red color wash and PTV was covered by 50.4 Gy (green line). The involved para-aortic lymph nodal PTV is depicted in blue color wash. (D) Showing left transposed ovarian covered by orange color wash and right covered by purple color wash (V7≤50%). (E) Sagittal and (F) coronal image showing PTV (red color wash) covered by 100% isodose line (green line, 50.4 Gy).

Fig. 2 The dose-volume histogram of the extended field intensity-modulated radiotherapy plan. The rectum and the bladder, V45≤50%, respectively; the small intestine, V35≤45%; the kidney received, V25≤33%; the liver, V30≤30%; the bone marrow, V10≤90% and V35≤45%; the ovarian, V7≤50%; the spinal cord, V40≤0.1 cubic centimeters.
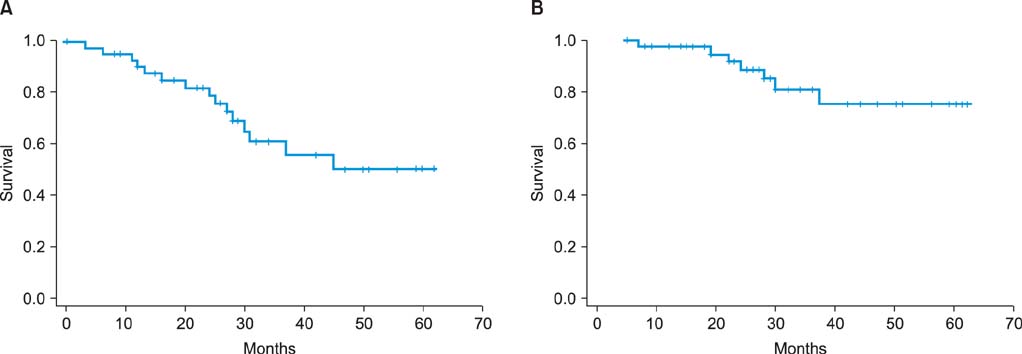
Fig. 3 (A) Kaplan-Meier graph showing disease-free survival. (B) Kaplan-Meier graph showing overall survival.
Reference
-
1. Keys HM, Bundy BN, Stehman FB, Muderspach LI, Chafe WE, Suggs CL 3rd, et al. Cisplatin, radiation, and adjuvant hysterectomy compared with radiation and adjuvant hysterectomy for bulky stage IB cervical carcinoma. N Engl J Med. 1999; 340:1154–1161.2. Lukka H, Hirte H, Fyles A, Thomas G, Elit L, Johnston M, et al. Concurrent cisplatin-based chemotherapy plus radiotherapy for cervical cancer: a meta-analysis. Clin Oncol (R Coll Radiol). 2002; 14:203–212.3. Morris M, Eifel PJ, Lu J, Grigsby PW, Levenback C, Stevens RE, et al. Pelvic radiation with concurrent chemotherapy compared with pelvic and para-aortic radiation for high-risk cervical cancer. N Engl J Med. 1999; 340:1137–1143.4. Grigsby PW, Siegel BA, Dehdashti F. Lymph node staging by positron emission tomography in patients with carcinoma of the cervix. J Clin Oncol. 2001; 19:3745–3749.5. Berman ML, Keys H, Creasman W, DiSaia P, Bundy B, Blessing J. Survival and patterns of recurrence in cervical cancer metastatic to periaortic lymph nodes (a Gynecologic Oncology Group study). Gynecol Oncol. 1984; 19:8–16.6. Piver MS, Barlow JJ, Krishnamsetty R. Five-year survival (with no evidence of disease) in patients with biopsy-confirmed aortic node metastasis from cervical carcinoma. Am J Obstet Gynecol. 1981; 139:575–578.7. Lovecchio JL, Averette HE, Donato D, Bell J. 5-year survival of patients with periaortic nodal metastases in clinical stage IB and IIA cervical carcinoma. Gynecol Oncol. 1989; 34:43–45.8. Nori D, Valentine E, Hilaris BS. The role of paraaortic node irradiation in the treatment of cancer of the cervix. Int J Radiat Oncol Biol Phys. 1985; 11:1469–1473.9. Rotman M, Pajak TF, Choi K, Clery M, Marcial V, Grigsby PW, et al. Prophylactic extended-field irradiation of para-aortic lymph nodes in stages IIB and bulky IB and IIA cervical carcinomas: ten-year treatment results of RTOG 79-20. JAMA. 1995; 274:387–393.10. Eifel PJ, Winter K, Morris M, Levenback C, Grigsby PW, Cooper J, et al. Pelvic irradiation with concurrent chemotherapy versus pelvic and para-aortic irradiation for high-risk cervical cancer: an update of radiation therapy oncology group trial (RTOG) 90-01. J Clin Oncol. 2004; 22:872–880.11. Grigsby PW, Heydon K, Mutch DG, Kim RY, Eifel P. Long-term follow-up of RTOG 92-10: cervical cancer with positive paraaortic lymph nodes. Int J Radiat Oncol Biol Phys. 2001; 51:982–987.12. Sood BM, Gorla GR, Garg M, Anderson PS, Fields AL, Runowicz CD, et al. Extended-field radiotherapy and high-dose-rate brachytherapy in carcinoma of the uterine cervix: clinical experience with and without concomitant chemotherapy. Cancer. 2003; 97:1781–1788.13. Kim YS, Kim JH, Ahn SD, Lee SW, Shin SS, Nam JH, et al. High-dose extended-field irradiation and high-dose-rate brachytherapy with concurrent chemotherapy for cervical cancer with positive paraaortic lymph nodes. Int J Radiat Oncol Biol Phys. 2009; 74:1522–1528.14. Jensen LG, Hasselle MD, Rose BS, Nath SK, Hasan Y, Scanderbeg DJ, et al. Outcomes for patients with cervical cancer treated with extended-field intensity-modulated radiation therapy and concurrent cisplatin. Int J Gynecol Cancer. 2013; 23:119–125.15. Portelance L, Chao KS, Grigsby PW, Bennet H, Low D. Intensity-modulated radiation therapy (IMRT) reduces small bowel, rectum, and bladder doses in patients with cervical cancer receiving pelvic and para-aortic irradiation. Int J Radiat Oncol Biol Phys. 2001; 51:261–266.16. Stryker JA, Mortel R. Survival following extended field irradiation in carcinoma of cervix metastatic to para-aortic lymph nodes. Gynecol Oncol. 2000; 79:399–405.17. Haie C, Pejovic MH, Gerbaulet A, Horiot JC, Pourquier H, Delouche J, et al. Is prophylactic para-aortic irradiation worthwhile in the treatment of advanced cervical carcinoma? Results of a controlled clinical trial of the EORTC radiotherapy group. Radiother Oncol. 1988; 11:101–112.18. Varia MA, Bundy BN, Deppe G, Mannel R, Averette HE, Rose PG, et al. Cervical carcinoma metastatic to para-aortic nodes: extended field radiation therapy with concomitant 5-fluorouracil and cisplatin chemotherapy: a Gynecologic Oncology Group study. Int J Radiat Oncol Biol Phys. 1998; 42:1015–1023.19. Ring KL, Young JL, Dunlap NE, Andersen WA, Schneider BF. Extended-field radiation therapy with whole pelvis radiotherapy and cisplatin chemosensitization in the treatment of IB2-IIIB cervical carcinoma: a retrospective review. Am J Obstet Gynecol. 2009; 201:109.e1–109.e6.20. Uno T, Mitsuhashi A, Isobe K, Yamamoto S, Kawakami H, Ueno N, et al. Concurrent daily cisplatin and extended-field radiation therapy for carcinoma of the cervix. Int J Gynecol Cancer. 2008; 18:80–84.21. Gerszten K, Colonello K, Heron DE, Lalonde RJ, Fitian ID, Comerci JT, et al. Feasibility of concurrent cisplatin and extended field radiation therapy (EFRT) using intensity-modulated radiotherapy (IMRT) for carcinoma of the cervix. Gynecol Oncol. 2006; 102:182–188.22. Lujan AE, Mundt AJ, Yamada SD, Rotmensch J, Roeske JC. Intensity-modulated radiotherapy as a means of reducing dose to bone marrow in gynecologic patients receiving whole pelvic radiotherapy. Int J Radiat Oncol Biol Phys. 2003; 57:516–521.23. Mell LK, Kochanski JD, Roeske JC, Haslam JJ, Mehta N, Yamada SD, et al. Dosimetric predictors of acute hematologic toxicity in cervical cancer patients treated with concurrent cisplatin and intensity-modulated pelvic radiotherapy. Int J Radiat Oncol Biol Phys. 2006; 66:1356–1365.24. Kodaira T, Fuwa N, Nakanishi T, Tachibana H, Nakamura T, Tomita N, et al. Prospective study of alternating chemoradiotherapy consisting of extended-field dynamic conformational radiotherapy and systemic chemotherapy using 5-FU and nedaplatin for patients in high-risk group with cervical carcinoma. Int J Radiat Oncol Biol Phys. 2009; 73:251–258.25. Chung YL, Jian JJ, Cheng SH, Hsieh CI, Tan TD, Chang HJ, et al. Extended-field radiotherapy and high-dose-rate brachytherapy with concurrent and adjuvant cisplatin-based chemotherapy for locally advanced cervical cancer: a phase I/II study. Gynecol Oncol. 2005; 97:126–135.26. Malfetano JH, Keys H, Cunningham MJ, Gibbons S, Ambros R. Extended field radiation and cisplatin for stage IIB and IIIB cervical carcinoma. Gynecol Oncol. 1997; 67:203–207.27. Chen SW, Liang JA, Hung YC, Yeh LS, Chang WC, Lin WC, et al. Concurrent weekly cisplatin plus external beam radiotherapy and high-dose rate brachytherapy for advanced cervical cancer: a control cohort comparison with radiation alone on treatment outcome and complications. Int J Radiat Oncol Biol Phys. 2006; 66:1370–1377.28. Beriwal S, Gan GN, Heron DE, Selvaraj RN, Kim H, Lalonde R, et al. Early clinical outcome with concurrent chemotherapy and extended-field, intensity-modulated radiotherapy for cervical cancer. Int J Radiat Oncol Biol Phys. 2007; 68:166–171.29. Morice P, Castaigne D, Haie-Meder C, Pautier P, El Hassan J, Duvillard P, et al. Laparoscopic ovarian transposition for pelvic malignancies: indications and functional outcomes. Fertil Steril. 1998; 70:956–960.30. Bidzinski M, Lemieszczuk B, Zielinski J. Evaluation of the hormonal function and features of the ultrasound picture of transposed ovary in cervical cancer patients after surgery and pelvic irradiation. Eur J Gynaecol Oncol. 1993; 14:Suppl. 77–80.31. Morice P, Juncker L, Rey A, El-Hassan J, Haie-Meder C, Castaigne D. Ovarian transposition for patients with cervical carcinoma treated by radiosurgical combination. Fertil Steril. 2000; 74:743–748.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effect of Radiation Therapy Techniques on Outcome in N3-positive IIIB Non-small Cell Lung Cancer Treated with Concurrent Chemoradiotherapy
- Present status of worldwide clinical trials about uterine cervical cancer
- Intensity-Modulated Radiation Therapy for Uterine Cervical Cancer to Reduce Toxicity and Enhance Efficacy – an Option or a Must?: A Narrative Review
- Is the Use of Intensity-Modulated Radiotherapy Beneficial for Pancreatic Cancer Patients?
- Radiation therapy of cervical cancer: Current status in Korea and recent developments
