Cancer Res Treat.
2016 Jan;48(1):106-114. 10.4143/crt.2014.131.
Effect of Radiation Therapy Techniques on Outcome in N3-positive IIIB Non-small Cell Lung Cancer Treated with Concurrent Chemoradiotherapy
- Affiliations
-
- 1Department of Radiation Oncology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. ahnyc@skku.edu
- KMID: 2152266
- DOI: http://doi.org/10.4143/crt.2014.131
Abstract
- PURPOSE
This study was conducted to evaluate clinical outcomes following definitive concurrent chemoradiotherapy (CCRT) for patients with N3-positive stage IIIB (N3-IIIB) non-small cell lung cancer (NSCLC), with a focus on radiation therapy (RT) techniques.
MATERIALS AND METHODS
From May 2010 to November 2012, 77 patients with N3-IIIB NSCLC received definitive CCRT (median, 66 Gy). RT techniques were selected individually based on estimated lung toxicity, with 3-dimensional conformal RT (3D-CRT) and intensity-modulated RT (IMRT) delivered to 48 (62.3%) and 29 (37.7%) patients, respectively. Weekly docetaxel/paclitaxel plus cisplatin (67, 87.0%) was the most common concurrent chemotherapy regimen.
RESULTS
The median age and clinical target volume (CTV) were 60 years and 288.0 cm3, respectively. Patients receiving IMRT had greater disease extent in terms of supraclavicular lymph node (SCN) involvement and CTV > or = 300 cm3. The median follow-up time was 21.7 months. Fortyfive patients (58.4%) experienced disease progression, most frequently distant metastasis (39, 50.6%). In-field locoregional control, progression-free survival (PFS), and overall survival (OS) rates at 2 years were 87.9%, 38.7%, and 75.2%, respectively. Although locoregional control was similar between RT techniques, patients receiving IMRT had worse PFS and OS, and SCN metastases from the lower lobe primary tumor and CTV > or = 300 cm3were associated with worse OS. The incidence and severity of toxicities did not differ significantly between RT techniques.
CONCLUSION
IMRT could lead to similar locoregional control and toxicity, while encompassing a greater disease extent than 3D-CRT. The decision to apply IMRT should be made carefully after considering oncologic outcomes associated with greater disease extent and cost.
Keyword
MeSH Terms
Figure
-
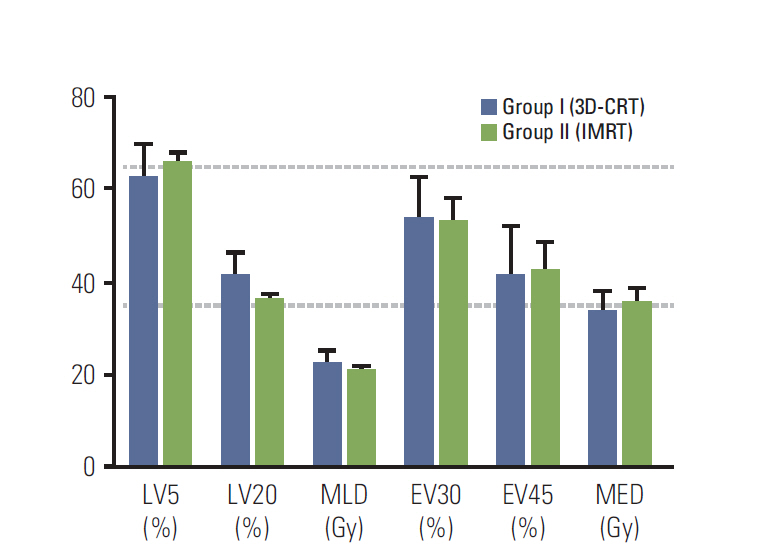
Fig. 1. Dose-volume parameters for lung and esophagus in patients with supraclavicular lymph node (SCN) originating from a lower lobe primary tumor. 3D-CRT, 3-dimensional conformal radiation therapy; IMRT, intensity-modulated radiation therapy; LV5 and LV20, volumes of the normal lung received ≥ 5 Gy and ≥ 20 Gy; MLD, mean lung dose; EV30 and EV45, volumes of the normal esophagus received ≥ 30 Gy and ≥ 45 Gy; MED, mean esophagus dose. Data are presented as the mean±standard error.
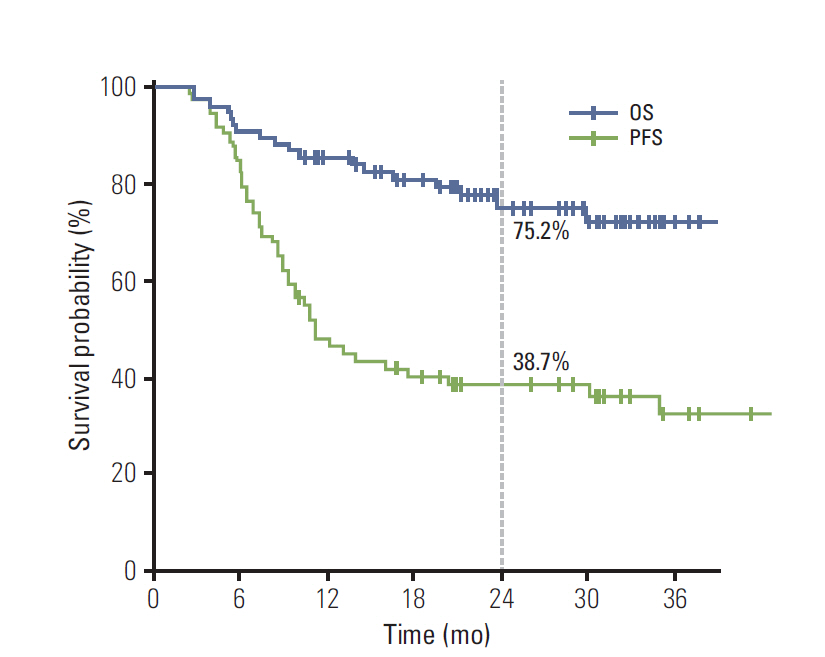
Fig. 2. Progression-free survival (PFS) and overall survival (OS) after definitive concurrent chemoradiotherapy in patients with N3-positive stage IIIB non-small cell lung cancer.
Reference
-
References
1. National Comprehensive Cancer Network. NCCN guidelines version 3, 2014. Non-small cell lung cancer [Internet] . Fort Washington, PA: National Comprehensive Cancer Network;2014. [cited 2014 May 28] . Available from: http://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf.2. Auperin A, Le Pechoux C, Rolland E, Curran WJ, Furuse K, Fournel P, et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J Clin Oncol. 2010; 28:2181–90.3. Curran WJ Jr, Paulus R, Langer CJ, Komaki R, Lee JS, Hauser S, et al. Sequential vs. concurrent chemoradiation for stage III non-small cell lung cancer: randomized phase III trial RTOG 9410. J Natl Cancer Inst. 2011; 103:1452–60.
Article4. Ramnath N, Dilling TJ, Harris LJ, Kim AW, Michaud GC, Balekian AA, et al. Treatment of stage III non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013; 143(5 Suppl):e314S–40S.5. Machtay M, Bae K, Movsas B, Paulus R, Gore EM, Komaki R, et al. Higher biologically effective dose of radiotherapy is associated with improved outcomes for locally advanced non-small cell lung carcinoma treated with chemoradiation: an analysis of the Radiation Therapy Oncology Group. Int J Radiat Oncol Biol Phys. 2012; 82:425–34.
Article6. Schallenkamp JM, Miller RC, Brinkmann DH, Foote T, Garces YI. Incidence of radiation pneumonitis after thoracic irradiation: dose-volume correlates. Int J Radiat Oncol Biol Phys. 2007; 67:410–6.
Article7. Oh D, Ahn YC, Park HC, Lim DH, Han Y. Prediction of radiation pneumonitis following high-dose thoracic radiation therapy by 3 Gy/fraction for non-small cell lung cancer: analysis of clinical and dosimetric factors. Jpn J Clin Oncol. 2009; 39:151–7.
Article8. Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. AJCC cancer staging manual. 7th ed. New York: Springer;2009.9. Grills IS, Yan D, Martinez AA, Vicini FA, Wong JW, Kestin LL. Potential for reduced toxicity and dose escalation in the treatment of inoperable non-small-cell lung cancer: a comparison of intensity-modulated radiation therapy (IMRT), 3D conformal radiation, and elective nodal irradiation. Int J Radiat Oncol Biol Phys. 2003; 57:875–90.
Article10. Liu HH, Wang X, Dong L, Wu Q, Liao Z, Stevens CW, et al. Feasibility of sparing lung and other thoracic structures with intensity-modulated radiotherapy for non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2004; 58:1268–79.
Article11. Murshed H, Liu HH, Liao Z, Barker JL, Wang X, Tucker SL, et al. Dose and volume reduction for normal lung using intensity-modulated radiotherapy for advanced-stage non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2004; 58:1258–67.
Article12. Yom SS, Liao Z, Liu HH, Tucker SL, Hu CS, Wei X, et al. Initial evaluation of treatment-related pneumonitis in advancedstage non-small-cell lung cancer patients treated with concurrent chemotherapy and intensity-modulated radiotherapy. Int J Radiat Oncol Biol Phys. 2007; 68:94–102.
Article13. Liao ZX, Komaki RR, Thames HD Jr, Liu HH, Tucker SL, Mohan R, et al. Influence of technologic advances on outcomes in patients with unresectable, locally advanced non-small-cell lung cancer receiving concomitant chemoradiotherapy. Int J Radiat Oncol Biol Phys. 2010; 76:775–81.
Article14. Jiang ZQ, Yang K, Komaki R, Wei X, Tucker SL, Zhuang Y, et al. Long-term clinical outcome of intensity-modulated radiotherapy for inoperable non-small cell lung cancer: the MD Anderson experience. Int J Radiat Oncol Biol Phys. 2012; 83:332–9.
Article15. Shirvani SM, Jiang J, Gomez DR, Chang JY, Buchholz TA, Smith BD. Intensity modulated radiotherapy for stage III non-small cell lung cancer in the United States: predictors of use and association with toxicities. Lung Cancer. 2013; 82:252.
Article16. Song CH, Pyo H, Moon SH, Kim TH, Kim DW, Cho KH. Treatment-related pneumonitis and acute esophagitis in non-small-cell lung cancer patients treated with chemotherapy and helical tomotherapy. Int J Radiat Oncol Biol Phys. 2010; 78:651.
Article17. Lee H, Ahn YC, Pyo H, Kim B, Oh D, Nam H, et al. Pretreatment clinical mediastinal nodal bulk and extent do not influence survival in N2-positive stage IIIA non-small cell lung cancer patients treated with trimodality therapy. Ann Surg Oncol. 2014; 21:2083–90.
Article18. Sura S, Gupta V, Yorke E, Jackson A, Amols H, Rosenzweig KE. Intensity-modulated radiation therapy (IMRT) for inoperable non-small cell lung cancer: the Memorial Sloan-Kettering Cancer Center (MSKCC) experience. Radiother Oncol. 2008; 87:17–23.
Article19. Ahn HK, Choi YL, Han JH, Ahn YC, Kim K, Kim J, et al. Epidermal growth factor receptor mutation and treatment outcome of mediastinoscopic N2 positive non-small cell lung cancer patients treated with neoadjuvant chemoradiotherapy followed by surgery. Lung Cancer. 2013; 79:300–6.
Article20. Ready N, Janne PA, Bogart J, Dipetrillo T, Garst J, Graziano S, et al. Chemoradiotherapy and gefitinib in stage III non-small cell lung cancer with epidermal growth factor receptor and KRAS mutation analysis: cancer and leukemia group B (CALEB) 30106, a CALGB-stratified phase II trial. J Thorac Oncol. 2010; 5:1382–90.
Article21. Blumenschein GR Jr, Paulus R, Curran WJ, Robert F, Fossella F, Werner-Wasik M, et al. Phase II study of cetuximab in combination with chemoradiation in patients with stage IIIA/B non-small-cell lung cancer: RTOG 0324. J Clin Oncol. 2011; 29:2312–8.
Article22. Shaw AT, Yeap BY, Solomon BJ, Riely GJ, Gainor J, Engelman JA, et al. Effect of crizotinib on overall survival in patients with advanced non-small-cell lung cancer harbouring ALK gene rearrangement: a retrospective analysis. Lancet Oncol. 2011; 12:1004–12.
Article23. Smith BD, Pan IW, Shih YC, Smith GL, Harris JR, Punglia R, et al. Adoption of intensity-modulated radiation therapy for breast cancer in the United States. J Natl Cancer Inst. 2011; 103:798–809.
Article24. Chino F, Peppercorn J, Taylor DH Jr, Lu Y, Samsa G, Abernethy AP, et al. Self-reported financial burden and satisfaction with care among patients with cancer. Oncologist. 2014; 19:414.
Article25. Zafar SY, Peppercorn JM, Schrag D, Taylor DH, Goetzinger AM, Zhong X, et al. The financial toxicity of cancer treatment: a pilot study assessing out-of-pocket expenses and the insured cancer patient's experience. Oncologist. 2013; 18:381–90.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Lack of the Difference in Outcome between N2 and N3 Non-Small Cell Lung Cancer Patients Treated with Concurrent Chemoradiotherapy; A Retrospective Analysis of 186 Patients
- Treatment Outcome of Locally Advanced Non-small Cell Lung Cancer
- Role of Radiation Therapy for Non-small Cell Lung Cancer: Focused on Stereotactic Ablative Radiation Therapy in Stage I
- Chemo-radiation Therapy for Locally Advanced Non-Small Cell Lung Cancer
- Early Result of Surgical Resection after Pre-Operative Concurrent chemoradiotherapy for N2-Positive Stage IIIA NSCLC
