Early-onset Childhood Sarcoidosis with Incidental Multiple Enchondromatosis
- Affiliations
-
- 1Department of Pediatrics, Wonkwang University Sanbon Medical Center, Gunpo, Korea.
- 2Department of Pediatrics, Chungnam University Hospital, Daejeon, Korea.
- 3Department of Radiology, Hanyang University Medical Center, Seoul, Korea.
- 4Department of Nuclear Medicine, Hanyang University Medical Center, Seoul, Korea.
- 5Department of Pathology, Hanyang University Medical Center, Seoul, Korea.
- 6Department of Pediatrics, Hanyang University Medical Center, Seoul, Korea. cord@hanyang.ac.kr
- KMID: 1792987
- DOI: http://doi.org/10.3346/jkms.2012.27.1.96
Abstract
- The triad of rash, arthritis, and uveitis seems to be characteristic for early-onset childhood sarcoidosis. We describe an interesting case of early-onset childhood sarcoidosis coexisting enchondromatosis, which clinically masquerade as Langerhans cell histiocytosis. A 33 months old girl presented with skin rash, subcutaneous nodules with polyarthritis, and revealed the involvement of lymph nodes as well as spleen during work-up. She also presented with multiple osteolytic lesions which pathologically proven enchondromatosis. Oral prednisone was prescribed at 2 mg/kg/day for 2 months until when subcutaneous nodules and joint swellings almost disappeared, and then slowly tapered over a period of 5 months. We report an unusual case of early-onset childhood sarcoidosis presented with osteolytic bone lesions which were irrelevant to sarcoidosis.
Keyword
MeSH Terms
-
Administration, Oral
Anti-Inflammatory Agents/therapeutic use
Arthritis/complications
Child, Preschool
Diagnosis, Differential
Enchondromatosis/*complications/*diagnosis/drug therapy/radiography
Exanthema/etiology
Female
Humans
Positron-Emission Tomography and Computed Tomography
Prednisone/therapeutic use
Sarcoidosis/*complications/*diagnosis/drug therapy/radiography
Whole Body Imaging
Figure
-

Fig. 1 Radiological images of the patient. (A) Multiple, small and elongated osteolytic lesions with thin sclerotic rims are noted in the both femoral necks (arrows). Both knee AP (B) and lateral views (C, D) show small, eccentric osteolytic lesions involving right proximal fibula and left proximal fibula (white arrows). Large amount of suprapatellar effusions are also noted in the both sides of knee (black lined white arrows). Both ankle AP (E) and right lateral views (F) show well-defined osteolytic lesions with thin sclerotic rim involving right distal fibula (white arrows) and left distal tibia (black lined white arrows).
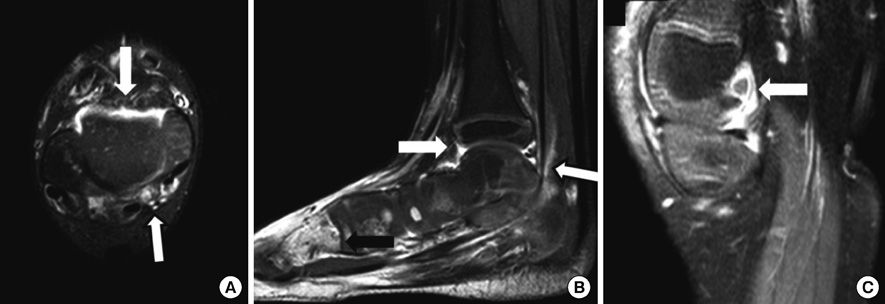
Fig. 2 MR scan images of low extremity. Contrast enhancement T1-weighted axial (A) and sagittal scans (B) with fat-suppression show diffuse synovial enhancement (white arrows) and tenosynovitis (black lined white arrows) around right ankle joint. Abnormal enhancement lesion is also noted in the right 2nd metatarsal shaft (black arrow). Contrast enhancement T1-weighted sagittal scans (C) with fat-suppression show joint effusion with diffuse synovial enhancement (white arrow) in the left tibia MR scans.

Fig. 3 The whole body bone scan showed no definite abnormal focal bony uptake lesions except mildly increased soft tissue uptake on the bilateral suprapatellar bursa area (arrows).
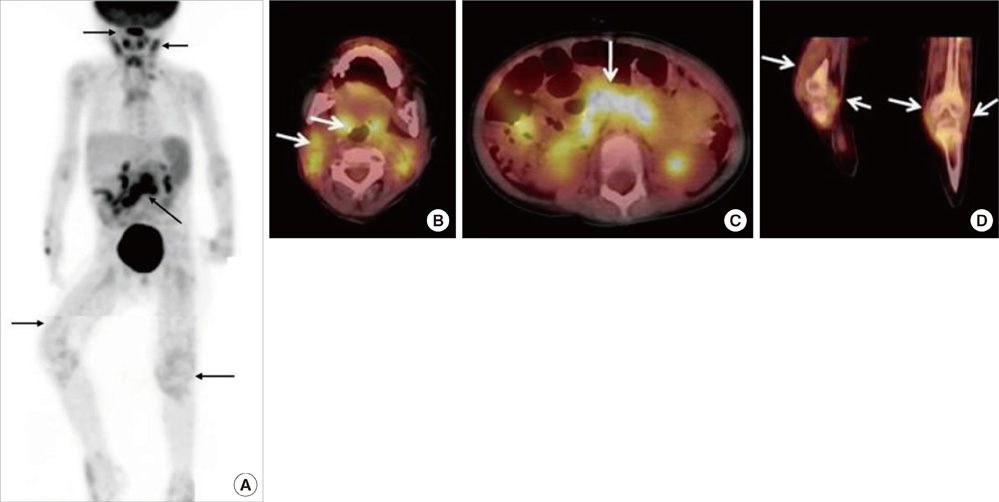
Fig. 4 PET/CT images. (A) Whole body MIP (maximum intensity projection) image. (B) Regional images demonstrating hypermetabolic activity in nasopharynx, bilateral tonsils and cervical lymph nodes. (C) Mid abdominal lymph nodes. (D) Thickened synovial lining of both knee joints.

Fig. 5 Histopathological findings of the biopsied tissue. Non-caseating, sarcoidal, chronic granulomatous inflammation is observed in the skin rash (A) and subcutaneous nodule, and synovium of knee joint (B, C). However, the pathological finding of right tibia is compatible with enchondroma (D). (H&E stained, A × 200; B, × 100; C and D, × 200).
Cited by 1 articles
-
Pediatric Sarcoidosis Misdiagnosed as Hepatosplenic Abscesses: A Case Report and Review
Su Min Lee, Hyungwook Choi, Sungmin Lim, Jehee Shin, Ji-Man Kang, Jong Gyun Ahn
J Rheum Dis. 2022;29(3):181-186. doi: 10.4078/jrd.2022.29.3.181.
Reference
-
1. Hunninghake GW, Costabel U, Ando M, Baughman R, Cordier JF, du Bois R, Eklund A, Kitaichi M, Lynch J, Rizzato G, Rose C, Selroos O, Semenzato G, Sharma OP. ATS/ERS/WASOG statement of sarcoidosis. American Thoracic Society/European Respiratory Society/World Association of Sarcoidosis and other Granulomatous Disorders. Sarcoidosis Vasc Diffuse Lung Dis. 1999. 16:149–173.2. Hetherington S. Sarcoidosis in young children. Am J Dis Child. 1982. 136:13–15.3. Häfner R, Vogel P. Sarcoidosis of early onset. A challenge for the pediatric rheumatologist. Clin Exp Rheumatol. 1993. 11:685–691.4. Fink CW, Cimaz R. Early onset sarcoidosis: not a benign disease. J Rheumatol. 1997. 24:174–177.5. Pattishall EN, Kendig EL Jr. Sarcoidosis in children. Pediatr Pulmonol. 1996. 22:195–203.6. Mallory SB, Paller AS, Ginsburg BC, McCrossin ID, Abernathy R. Sarcoidosis in children: differentiation from juvenile rheumatoid arthritis. Pediatr Dermatol. 1987. 4:313–319.7. Rosenberg AM, Yee EH, MacKenzie JW. Arthritis in childhood sarcoidosis. J Rheumatol. 1983. 10:987–990.8. Hoffmann AL, Milman N, Byg KE. Childhood sarcoidosis in Denmark 1979-1994: incidence, clinical features and laboratory results at presentation in 48 children. Acta Paediatr. 2004. 93:30–36.9. Baculard A, Blanc N, Boulé M, Fauroux B, Chadelat K, Boccon-Gibod L, Tournier G, Clement A. Pulmonary sarcoidosis in children: a follow-up study. Eur Respir J. 2001. 17:628–635.10. Fauroux B, Clèment A. Paediatric sarcoidosis. Paediatr Respir Rev. 2005. 6:128–133.11. Kim DS. Sarcoidosis in Korea: report of the Second Nationwide Survey. Sarcoidosis Vasc Diffuse Lung Dis. 2001. 18:176–180.12. Aouba A, Larousserie F, Le Guern V, Martin A, Guillevin L. Spumous histiocytic oligoarthritis coexisting with systemic Langerhans' cell histiocytosis: case report and literature review. Joint Bone Spine. 2009. 76:701–704.13. Wilcox A, Bharadwaj P, Sharma OP. Bone sarcoidosis. Curr Opin Rheumatol. 2000. 12:321–330.14. Nishiyama Y, Yamamoto Y, Fukunaga K, Takinami H, Iwado Y, Satoh K, Ohkawa M. Comparative evaluation of 18F-FDG PET and 67Ga scintigraphy in patients with sarcoidosis. J Nucl Med. 2006. 47:1571–1576.15. Teirstein AS, Machac J, Almeida O, Lu P, Padilla ML, Iannuzzi MC. Results of 188 whole-body fluorodeoxyglucose positron emission tomography scans in 137 patients with sarcoidosis. Chest. 2007. 132:1949–1953.16. Zhuang H, Alavi A. 18-fluorodeoxyglucose positron emission tomographic imaging in the detection and monitoring of infection and inflammation. Semin Nucl Med. 2002. 32:47–59.
