A Case of Pseudoalveolar Sarcoidosis with Unilateral Pulmonary Infiltration
- Affiliations
-
- 1Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea. droij@chonnam.ac.kr
Abstract
- A sarcoidosis is a multisystemic granulomatous disorder that has a predilection for pulmonary involvement, and the common radiological findings for the disease are bilateral nodular or reticulonodular patterns. Pseudoalveolar sarcoidosis is a rare presentation of sarcoidosis. The radiological finding is an alveolar pattern that involves or compresses the alveoli by clustered interstitial granuloma. A 58-year-old man was admitted due to incidental findings of a unilateral consolidative lesion as seen on chest radiography. A chest computed tomography (CT) examination showed multiple bronchoalveolar consolidations that were suspicious of a malignancy. However, a percutaneous needle biopsy revealed non-caseating granuloma with an asteroid body that was compatible with sarcoidosis. After one month, the consolidative lesions improved without any treatment.
Keyword
Figure
-
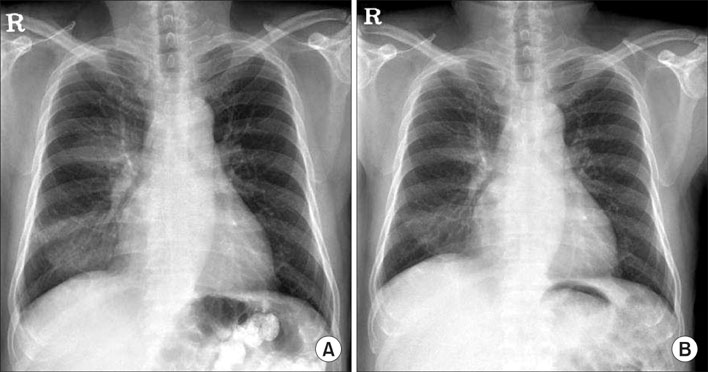
Figure 1 (A) Initial chest X-ray shows a consolidation of the right lower lung field. (B) A follow-up chest X-ray (1 month later) shows a partial resolution of consolidation of the right lower lung field.
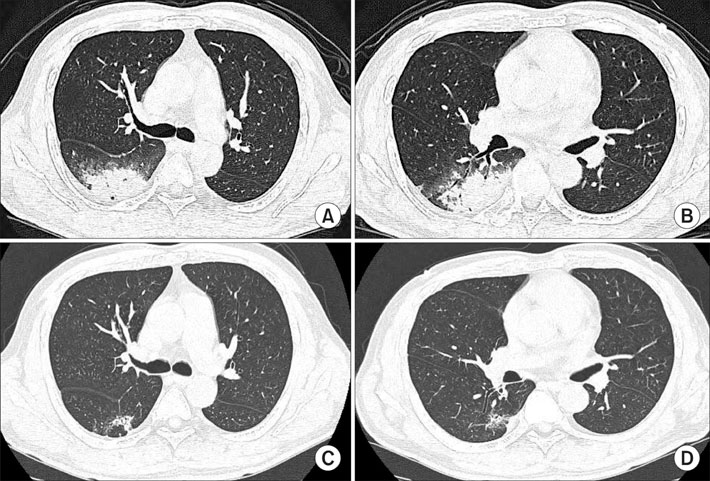
Figure 2 (A, B) Initial chest HRCT scans shows a mass-like opacity in the superior and posterobasal segment of the right lower lobe. (C, D) Follow-up chest HRCT (4 months later) scans shows a resolution of previous lesions in the superior and posterobasal segment of the right lower lobe.
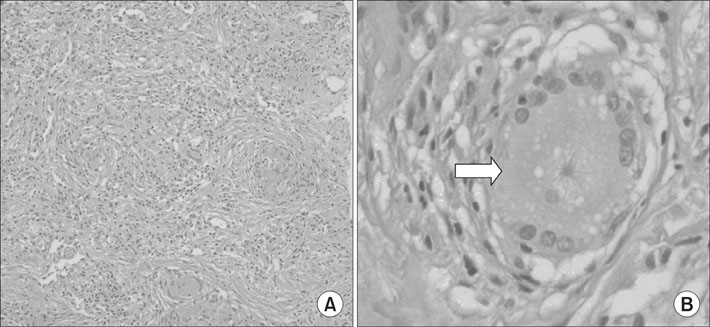
Figure 3 The pathologic findings of transthoracic needle biopsy reveals (A) chronic non-caseatng granulomatous inflammation and giant cell (H&E stain, ×200). (B) In high power field, there is a asteroid body (white arrow) in giant cell (H&E stain, ×400).
Reference
-
1. Johkoh T, Ikezoe J, Takeuchi N, Kohno N, Tomiyama N, Akira M, et al. CT findings in "pseudoalveolar" sarcoidosis. J Comput Assist Tomogr. 1992. 16:904–907.2. Muller NL, Mawson JB, Mathieson JR, Abboud R, Ostrow DN, Champion P. Sarcoidosis: correlation of extent of disease at CT with clinical, functional, and radiographic findings. Radiology. 1989. 171:613–618.3. Sahn SA, Schwarz MI, Lakshminarayan S. Sarcoidosis: the significance of an acinar pattern on chest roentgenogram. Chest. 1974. 65:684–687.4. Grenier P, Valeyre D, Cluzel P, Brauner MW, Lenoir S, Chastang C. Chronic diffuse interstitial lung disease: diagnostic value of chest radiography and high-resolution CT. Radiology. 1991. 179:123–132.5. Battesti JP, Saumon G, Valeyre D, Amouroux J, Pechnick B, Sandron D, et al. Pulmonary sarcoidosis with an alveolar radiographic pattern. Thorax. 1982. 37:448–452.6. Nam JE, Ryu YH, Park JG, Choe KO, Im JG, Lee KS, et al. High resolution CT findings of pseudoalveolar sarcoidosis. J Korean Radiol Soc. 2002. 47:191–196.7. Hamper UM, Fishman EK, Khouri NF, Johns CJ, Wang KP, Siegelman SS. Typical and atypical CT manifestation of pulmonary sarcoidosis. J Comput Assist Tomogr. 1986. 10:928–936.8. Sharma OP. Sarcoidosis: a worldwide phenomenon. Sarcoidosis. 1984. 1:11–15.9. Brauner MW, Grenier P, Mompoint D, Lenoir S, de Cremoux H. Pulmonary sarcoidosis: evaluation with high resolution CT. Radiology. 1989. 172:467–471.10. Gibson GJ, Prescott RJ, Muers MF, Middleton WG, Mitchell DN, Connolly CK, et al. British Thoracic Society Sarcoidosis study: effects of long term corticosteroid treatment. Thorax. 1996. 51:238–247.11. Newman LS, Rose CS, Maier LA. Sarcoidosis. N Engl J Med. 1997. 336:1224–1234.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Subcutaneous Sarcoidosis of the Distal Lower Leg in a Middle-Aged Woman Associated with Pulmonary Sarcoidosis: a Case Report
- A Case of Cutaneous Sarcoidosis in the Mucosal Membrane of the Lower Lip
- A Case of Pulmonary Sarcoidosis in a 6-year-old Girl
- High Resolution CT Findings of Pseudoalveolar Sarcoidosis
- A Case of Ichthyosiform Sarcoidosis
