J Korean Endocr Soc.
2006 Oct;21(5):424-427. 10.3803/jkes.2006.21.5.424.
A Case of Spontaneous Rupture of Adrenal Pheochromocytoma
- Affiliations
-
- 1Department of Internal Medicine, Inha University, College of Medicine, Korea.
- 2Department of Pathology, Inha University, College of Medicine, Korea.
- KMID: 1511994
- DOI: http://doi.org/10.3803/jkes.2006.21.5.424
Abstract
- Although the spontaneous rupture of a pheochromocytoma is rare, it can be fatal if not promptly diagnosed. Hemorrhagic necrosis of the tumor will require an emergency operation, as this causes intraperitoneal hemorrhaging. Excessive vasoconstriction, tachycardia and labile blood pressure are the signs of a ruptured pheochromocytoma. The standard diagnostic tool of such a condition is an abdominal computed tomographic scan. Although the exact mechanism of the rupture is still unknown, a hemorrhage inside the tumor or a high intra-cortical pressure, due to rapid growth of the tumor, is known to play a major role in the pathogenesis. Herein is reported the case of a 53-year old male patient with a pheochromocytoma and an acute abdomen. The CT scan showed a left adrenal gland mass, with a hemorrhage in the left perirenal space. The patient underwent an emergency adrenalectomy, with the final histopathological diagnosis being that of a pheochromocytoma. Prompt recognition and early surgical intervention can improve outcome.
Keyword
MeSH Terms
Figure
-
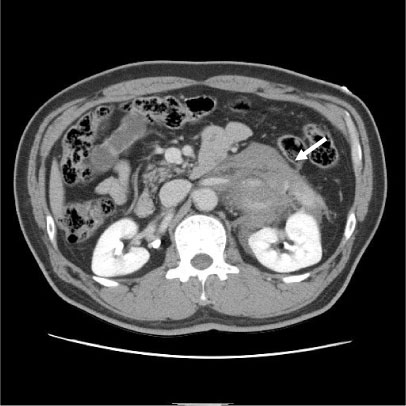
Fig. 1 Abdominal CT shows 6.2 × 1.3 cm sized adrenal mass with hemorrhage in left anterior pararenal and perirenal space.
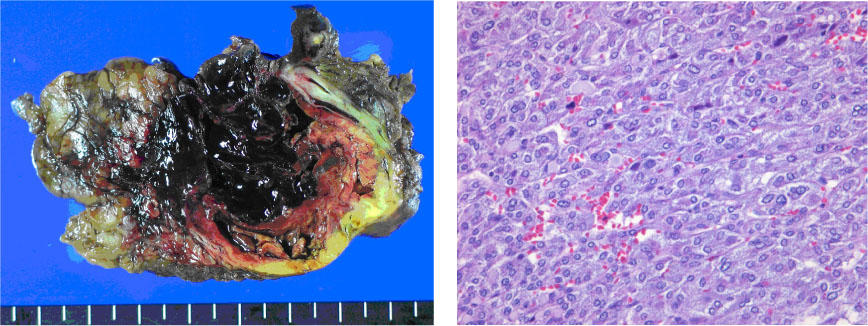
Fig. 2 A, Gross findings of tumor shows encaspulated and diffuse areas of hemorrhage; B, Microscopic finding of the tumor. Individual tumor cells have a finely granular basophilic or amphophilic cytoplasm with frequent hyaline globules. The nuclei of the tumor cells are round to oval with prominent nucleolus and occasional intranuclear cytoplasmic inclusion (H&E stain, × 400).
Reference
-
1. Tanaka K, Noguchi S, Shuin T, Kinoshita Y, Kubota Y, Hosaka M. Spontaneous rupture of adrenal pheochromocytoma: a case report. J Urol. 1994. 151:120–121.2. Sumino Y, Tasaki Y, Satoh F, Mimata H, Nomura Y. Spontaneous rupture of adrenal pheochromocytoma. J Urol. 2002. 168:188–189.3. Takashi K, Akira I, Ryo T, Yoshihiro I, Koji N, Kenji M. Spontaneous rupture of adrenal pheochromocytoma: review and analysis of prognostic factors. J Surg Oncol. 2005. 90:31–35.4. Larsen PR, Kronenberg HM, Melmed S, Polonsky KS. Williams textbook of endocrinology. 2002. 10th ed. Saunders;555–562.5. Chan MKY, Test HW, Mok FPT. Ruptured pheochromocytoma-a lesson in acute abdomen. Hong Kong Med J. 2003. 9:221–223.6. Greatorex RA, Raftery AT. Intraperitoneal rupture of a pheochoromocytoma. J R Soc Med. 1984. 77:513–514.7. Forty J, Dale RF. Ruptured pheochoromocytoma: a case report. J R Coll Surg Edinb. 1989. 34:109–110.8. Mayo-Smith WW, Boland GW, Noto RB, Lee MJ. State-of-the-art adrenal imaging. Radiographic. 2001. 21:995 –1012.9. Machuca Santa Cruz J, Julve Villalta E, Galacho Bech A, Perez Rodriguez D, Quinonero Diaz A, Alonzo Dorrego JM, Marin Martin JA. Spontaneous retroperitoneal hematoma: our experience. Actas Urol Esp. 1999. 23:43–50.10. Sapienza P, Tedesco M, Graziano P, Moretti M, Mingazzini PL, Cavallaro A. An unusual case of spontaneous rupture of a clinically "silent" pheochromocytoma. Anticancer Res. 1997. 17:717–720.11. Suzuki K. Surgical management of pheochoromocytoma. Biomed Pharmacother. 2000. 54:suppl 1. S150–S156.12. Prys-Roberts C. Pheochromocytoma-recent progress in its management. Br J Anaesth. 2000. 85:44–57.
