A Case of Primary Hyperparathyroidism Caused by Solitary Parathyroid Adenoma That was Not Detected by Both Ultrasonography and Sestamibi Scan
- Affiliations
-
- 1Department of Internal Medicine, Gachon University School of Medicine, Incheon, Korea. shleemd@gachon.ac.kr
- 2Department of Nuclear Medicine, Gachon University School of Medicine, Incheon, Korea.
- 3Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- 4Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1497725
- DOI: http://doi.org/10.3803/EnM.2011.26.2.166
Abstract
- Thanks to advances in assay techniques and routine measurements in serum chemical analysis, primary hyperparathyroidism has become far more frequently detected, and the number of asymptomatic patients has substantially increased. In the majority of patients (85%), a solitary adenoma is the underlying cause of primary hyperparathyroidism. Surgical excision is the treatment of choice for most cases of primary hyperparathyroidism; this procedure has a relatively high success rate. In the past decade, improvements in preoperative imaging have played a major role in a targeted operative approach, which allows for minimally invasive surgery to be performed. The success of parathyroid surgery depends on the accurate preoperative localization of parathyroid adenoma. In this study, we report the case of a 54 year-old woman with primary hyperparathyroidism who presented with left buttock and leg pain. For localization of the parathyroid lesion, an ultrasonography and a 99mTc-sestamibi scan were initially performed, but these attempts failed to localize the lesion. We then carried out contrast-enhanced CT; thereafter, a single parathyroid adenoma was detected. Therefore, in patients with negative results on both ultrasonography and 99mTc-sestamibi scan, contrast-enhanced CT may prove helpful for preoperative parathyroid localization.
MeSH Terms
Figure
-
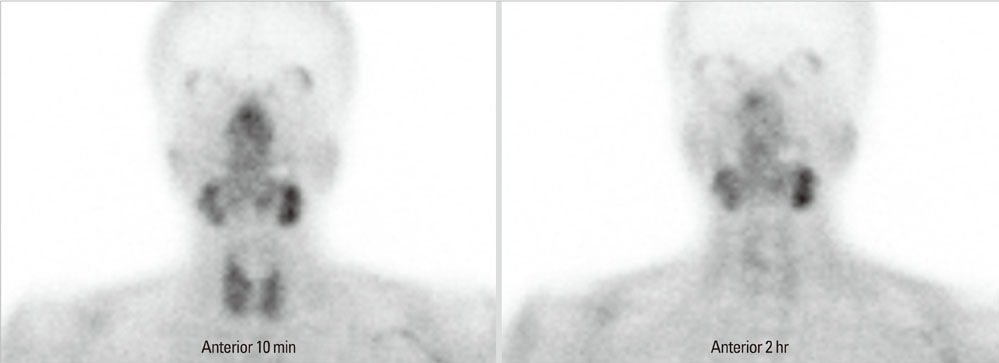
Fig. 1 99mTc-sestamibi scan shows no focal parathyroid uptake on 2-hour delayed image.
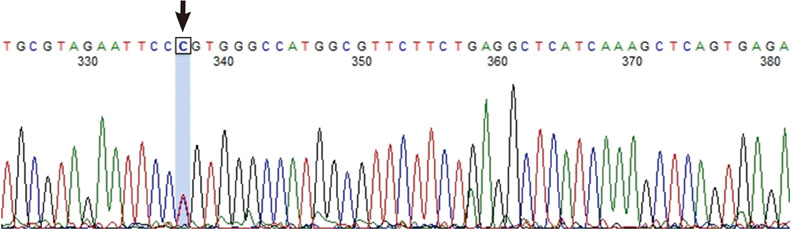
Fig. 2 Sequence chromatogram of parts of exon 7 of the CaSR gene from the proband. The arrow in the chromatogram indicates the presense of heterozygous missense nucleotide substitution due to T → C substitution at nucleotide 2968 causing R990G in the PCR with reverse primer.
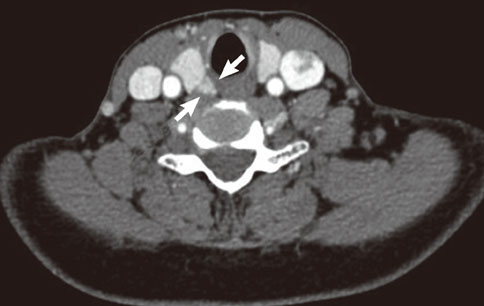
Fig. 3 Contrast-enhanced CT of lower neck shows a contrast enhancing lesion posterior to the right lobe of thyroid gland (arrows).
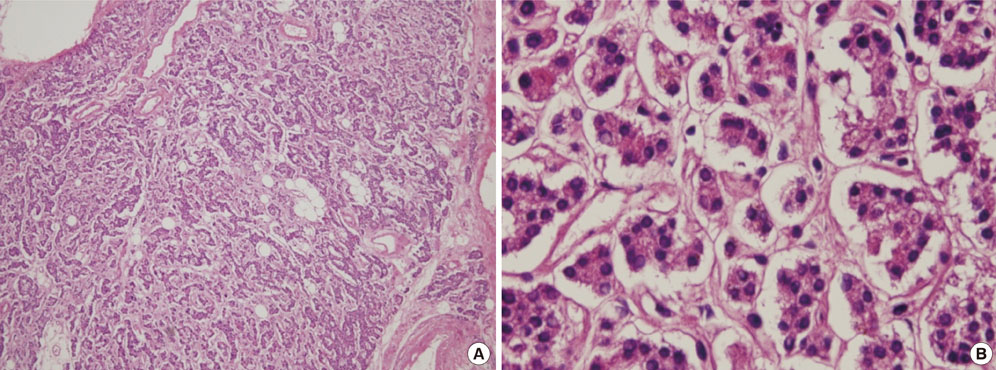
Fig. 4 Microscopic findings of parathyroid gland show homogenous proliferative lesions without vascular invasion. The chief cells are predominant and arranged in acinar pattern. Nuclei are small round and have finely dense chromatin with faintly eosinophilic cytoplasm, consistent with parathyroid adenoma (A, H&E stain; × 40; B, × 400).
Reference
-
1. Adami S, Marcocci C, Gatti D. Epidemiology of primary hyperparathyroidism in Europe. J Bone Miner Res. 2002. 17:Suppl 2. N18–N23.2. Chung HK, Kim DY, Woo JT, Kim SW, Yang IM, Kim JW, Kim YS, Kim KW, Choi YK. Review of clinical characteristics of primary hyperparathyroidism. J Korean Soc Endocrinol. 1992. 7:234–242.3. DeLellis R. Randolph GW, editor. Surgical pathology of the parathyoid glands. Surgery of the thyroid and parathyroid glands. 2003. Philadelphia: Saunders;571–577.4. Mandl F. Therapeutischer versuch bein falls von ostitis fibrosa generalisata mittles: extirpation eines epithelkorperchen tumors. Wien Klin Wochenshr. 1925. 50:1343.5. Delbridge LW, Younes NA, Guinea AI, Reeve TS, Clifton-Bligh P, Robinson BG. Surgery for primary hyperparathyroidism 1962-1996: indications and outcomes. Med J Aust. 1998. 168:153–156.6. Salti GI, Fedorak I, Yashiro T, Fulton N, Hara H, Yousefzadeh D, Kaplan EL. Continuing evolution in the operative management of primary hyperparathyroidism. Arch Surg. 1992. 127:831–836.7. Yen TW, Wang TS, Doffek KM, Krzywda EA, Wilson SD. Reoperative parathyroidectomy: an algorithm for imaging and monitoring of intraoperative parathyroid hormone levels that results in a successful focused approach. Surgery. 2008. 144:611–619.8. Ishibashi M, Nishida H, Hiromatsu Y, Kojima K, Uchida M, Hayabuchi N. Localization of ectopic parathyroid glands using technetium-99m sestamibi imaging: comparison with magnetic resonance and computed tomographic imaging. Eur J Nucl Med. 1997. 24:197–201.9. Heath H 3rd, Hodgson SF, Kennedy MA. Primary hyperparathyroidism. Incidence, morbidity, and potential economic impact in a community. N Engl J Med. 1980. 302:189–193.10. Bilezikian JP, Silverberg SJ, Shane E, Parisien M, Dempster DW. Characterization and evaluation of asymptomatic primary hyperparathyroidism. J Bone Miner Res. 1991. 6:Suppl 2. S85–S89.11. Udelsman R. Six hundred fifty-six consecutive explorations for primary hyperparathyroidism. Ann Surg. 2002. 235:665–670.12. Russell CF, Dolan SJ, Laird JD. Randomized clinical trial comparing scan-directed unilateral versus bilateral cervical exploration for primary hyperparathyroidism due to solitary adenoma. Br J Surg. 2006. 93:418–421.13. Ruda JM, Hollenbeak CS, Stack BC Jr. A systematic review of the diagnosis and treatment of primary hyperparathyroidism from 1995 to 2003. Otolaryngol Head Neck Surg. 2005. 132:359–372.14. Takami H, Oshima M, Sugawara I, Satake S, Ikeda Y, Nakamura K, Kubo A. Pre-operative localization and tissue uptake study in parathyroid imaging with technetium-99m-sestamibi. Aust N Z J Surg. 1999. 69:629–631.15. Palestro C, Tomas M, Tronco G. Radionuclide Imaging of the Parathyroid Glands. Seminars in Nuclear Medicine. 2005. 35:266–276.16. McHenry CR, Lee K, Saadey J, Neumann DR, Esselstyn CB Jr. Parathyroid localization with technetium-99m-sestamibi: a prospective evaluation. J Am Coll Surg. 1996. 183:25–30.17. Feingold DL, Alexander HR, Chen CC, Libutti SK, Shawker TH, Simonds WF, Marx SJ, Skarulis MC, Doppman JL, Schrump DS, Bartlett DL. Ultrasound and sestamibi scan as the only preoperative imaging tests in reoperation for parathyroid adenomas. Surgery. 2000. 128:1103–1109.18. Gotway MB, Higgins CB. MR imaging of the thyroid and parathyroid glands. Magn Reson Imaging Clin N Am. 2000. 8:163–182.19. Mariani G, Gulec SA, Rubello D, Boni G, Puccini M, Pelizzo MR, Manca G, Casara D, Sotti G, Erba P, Volterrani D, Giuliano AE. Preoperative localization and radioguided parathyroid surgery. J Nucl Med. 2003. 44:1443–1458.20. Corbetta S, Eller-Vainicher C, Filopanti M, Saeli P, Vezzoli G, Arcidiacono T, Loli P, Syren ML, Soldati L, Beck-Peccoz P, Spada A. R990G polymorphism of the calcium-sensing receptor and renal calcium excretion in patients with primary hyperparathyroidism. Eur J Endocrinol. 2006. 155:687–692.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Mediastinal parathyroid adenoma localized by technetium-99m sestamibi scanning
- Primary Hyperparathyroidism with Ectopic Parathyroid Adenoma Detected by Both 99mTc-MIBI SPECT and Contrast-Enhanced Neck CT
- A case of mediastinal parathyroid adenoma presenting as fracture of brown tumor
- Comparison of Ultrasonography and 99mTc-sestamibi Scan for Preoperative Localization of Parathyroid Adenoma
- Primary Hyperparathyroidism Caused by a Giant Parathyroid Adenoma: A case report
