J Korean Endocr Soc.
2009 Mar;24(1):42-46. 10.3803/jkes.2009.24.1.42.
Normal Repetitive Pregnancies and Tumor Regression Induced by Low-Dose Bromocriptine in a Patient with Macroprolactinoma
- Affiliations
-
- 1Department of Internal Medicine, Korea University College of Medicine, Korea.
- KMID: 1468495
- DOI: http://doi.org/10.3803/jkes.2009.24.1.42
Abstract
- Prolactin-secreting adenomas are the most common pituitary tumors. Menstrual disturbances and infertility are the main complaints in women with prolactinoma. Dopaminergic agonists such as bromocriptine are well-established treatments for prolactinoma when pregnancy is desired. Pregnancy-related outcomes in macroprolactinoma are worse than those in microprolactinoma. In addition, symptomatic tumor expansion during pregnancy occurs in 30% of women with macroprolactinoma. Therefore, when women with macroprolactinoma are planning a pregnancy, serum prolactin level should be normalized and the tumor volume significantly reduced. On the other hand, a spontaneous regression of macroprolactinoma can occur after pregnancy. We report a case of macroprolactinoma showing significant tumor regression during repeated pregnancies and low dose bromocriptine treatment, with a literature review.
Keyword
MeSH Terms
Figure
-
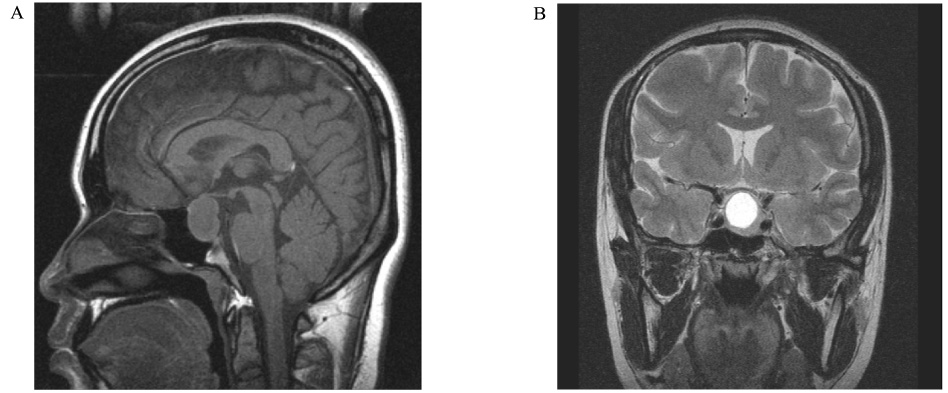
Fig. 1 Sellar MRI. The diameter of the tumor is 2.3 × 1.7 cm with suprasellar extension to compress optic chiasm. It is mainly cystic with high signal intensity on T2 weighted image (A. sagittal view. B. coronal view).

Fig. 2 Sellar MRI. No evidence of residual pituitary adenoma. Pituitary stalk deviated to right and a small T1 hyperintense nodule at the end of stalk which is thought to be abnormal developed neurohypophysis due to adenoma are showed (A. sagittal view. B. coronal view).
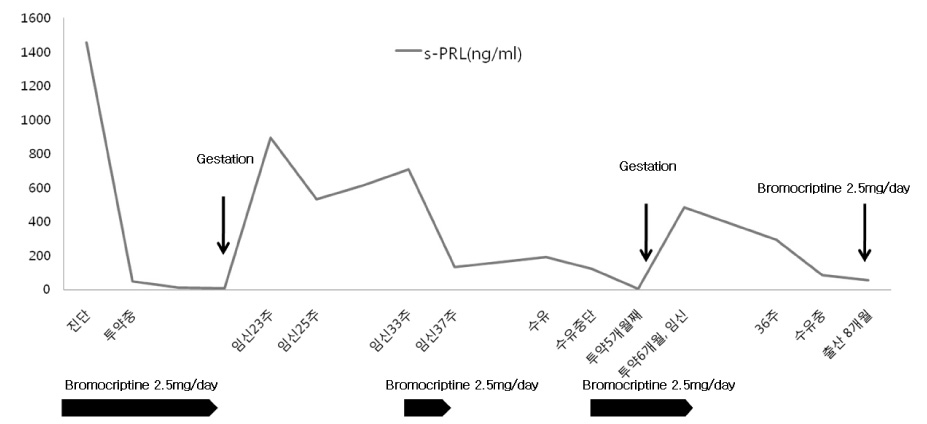
Fig. 3 Change in serum prolactin level during treatment and pregnancy.
Reference
-
1. Molitch ME. Pituitary incidentalomas. Endocrinol Metab Clin North Am. 1997. 26:725–740.2. Crosignani PG, Ferrar C, Scarduelli C, Picciotti MC, Caldara R, Malinverni A. Spontaneous and induced pregnancies in hyperprolactinemic women. Obstet Gynecol. 1981. 58:708–713.3. Cuellar FG. Bromocriptine mesylate (Parlodel) in the management of amenorrhea/galactorrhea associated with hyperprolactinemia. Obstet Gynecol. 1980. 55:278.4. Gemzell C, Wang CF. Outcome of pregnancy in women with pituitary adenoma. Fertil Steril. 1979. 31:363.5. Hardy J, Beauregard H, Robert F. Robyn , Harter M, editors. Prolactin secreting pituitary adenomas : transsphenoidal microsurgical treatment. Progress in Prolactin Physiology and Pathology. 1978. Amsterdam: Elesvier-North Holland Biomedical Press;361.6. Ahmed M, al-Dossary E, Woodhouse NJ. Macroprolactinomas with suprasellar extension: effect of bromocriptine withdrawal during one or more pregnancies. Fertil steril. 1992. 58:492–497.7. Mindermann T, Wilson CB. Age-related and gender-related occurrence of pituitary adenomas. Clin Endocrinol (Oxf). 1994. 41:359–364.8. Monroe SE, Levine L, Chang RJ, Keye WR Jr, Yamamoto M, Jaffe RB. Prolactin secreting pituitary adenomas: V. Increased gonadotropin responsivity in hyperprolactinemic women with pituitary adenomas. J Clin Endocrinol Metab. 1981. 52:1171.9. Hardy J. Transsphenoidal microsurgical removal of pituitary micro-adenoma. Prog Neurol Surg. 1975. 6:200–216.10. Serri O, Rasio E, Beauregard H, Hardy J, Somma M. Recurrence of hyperprolactinemia after selective transsphenoidal adenomectomy in women with prolactinoma. N Engl J Med. 1983. 309:280–283.11. Molitch ME, Elton RL, Blackwell RE, Caldwell B, Chang RJ, Jaffe R, Joplin G, Robbins RJ, Tyson J, Thorner MO. Bromocriptine as primary therapy for prolactin-secreting macroadenomas: Results of a prospective multicenter study. J Clin Endocrinol Metab. 1985. 60:698–705.12. Liuzzi A, Dallabonzana D, Oppizzi G, Verde GG, Cozzi R, Chiodini P, Luccarelli G. Low doses of dopamine agonists in the long-term treatment of macroprolactinomas. N Engl J Med. 1985. 313:656–659.13. Spark RF, Baker R, Bienfang DC, Bergland R. Bromocriptine reduces pituitary tumor size and hypersecretion. JAMA. 1982. 247:311.14. Trukalj I, Braun P, Krupp P. Surveillance of bromocriptine in pregnancy. JAMA. 1982. 247:1589–1591.15. Molitch ME. Management of prolactinomas during pregnancy. J Reprod Med. 1999. 44:1121–1126.16. Bronstein MD. Prolactinomas and pregnancy. Pituitary. 2005. 8:31–38.17. Essaïs O, Bouguerra R, Hamzaoui J, Marrakchi Z, Hadjri S, Chamakhi S, Zidi B, Ben Slama C. Efficacy and safety of bromocriptine in the treatment of macroprolactinomas. Ann Endocrinol (Paris). 2002. 63:524–531.18. Holmgren U, Bergstrand G, Hagenfeldt K, Werner S. Women with prolactinoma - effect of pregnancy and lactation on serum prolactin and on tumour growth. Acta Endocrinol. 1986. 111:452–458.19. Magyar DM, Marshall JR. Pituitary tumor and pregnancy. Am J Obstet Gynecol. 1978. 132:739.20. Bronstein MD, Salgado LR, de Castro Musolino NR. Medical management of pituitary adenomas: the special case of management of the pregnant woman. Pituitary. 2002. 5:99–107.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Preoperative Bromocriptine Treatment of the Large Pituitary Adenoma
- Comparison of Treatment Modalities in Hyperprolactinemia
- Effect of bromocriptine on 6-hydroxydopamine-induced lipid peroxidation and cytotoxicity in vitro and in vivo
- A Case of Bromocriptine Resistant Hyperprolactinemia Which was Responsive to Pergolide
- Treatment of Parkinson's Disease with Bromocriptine
