Serongative Acute Hepatic Failure-associated Aplastic Anemia in Pediatric Liver Transplantation
- Affiliations
-
- 1Department of Surgery, Seoul National University College of Medicine, Seoul, Korea. gsleenj@hanmail.net
- 2Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
- 3Department of Pediatrics, Seoul National University College of Medicine, Seoul, Korea.
- 4Department of Pathology, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 1450977
- DOI: http://doi.org/10.4285/jkstn.2011.25.4.276
Abstract
- Aplastic anemia (AA) is a rare complication of liver transplantation. The causes of AA have not yet been identified, and optimal treatment for AA after liver transplantation has not been firmly established. We experienced two cases of AA accompanied with fulminant hepatitis among 157 pediatric recipients (1.3%) and among 17 recipients of Korean Network of Organ Sharing (KONOS) status 1 (11.8%). The patients were a 16-year-old girl and a 3-year-old boy who had jaundice and lethargy due to non-A, non-B, non-C fulminant hepatitis. The girl underwent split liver transplantation involving the liver of a 24-year-old man, and the boy underwent an emergency living donor liver transplantation with a liver obtained from his 16-year-old cousin. Each transplantation procedure was uneventful. However, both patients were diagnosed with AA caused by thrombocytopenia and neutropenia at 140 and 26 days, respectively, after liver transplantation. The girl recovered completely after undergoing bone marrow transplantation and was followed up for 70 months. However, the boy was conservatively treated because of the development of hyperbilirubinemia and pyrexia. He died of multi-organ failure 74 days after liver transplantation. AA is not a rare complication of pediatric liver transplantation for fulminant hepatic failure. Therefore, AA must be suspected in pediatric cases of cytopenia even after liver transplantation. Our findings indicate bone marrow transplantation is the treatment of choice for AA even in cases where AA develops after liver transplantation.
Keyword
MeSH Terms
Figure
-

Fig. 1. Explant liver pathology of the patients suffered from fulminant hepatic failure. (A) Explant liver pathology of a 16-year-old girl suffered from fulminant hepatic failure (HE stain, ×200). (B) Explant liver pathology of a 3-year-old boy suffered from fulminant hepatic failure (HE stain, ×400). The explants liver shows submassive hepatic necrosis with diffuse lobular replacement by Herring ductules.
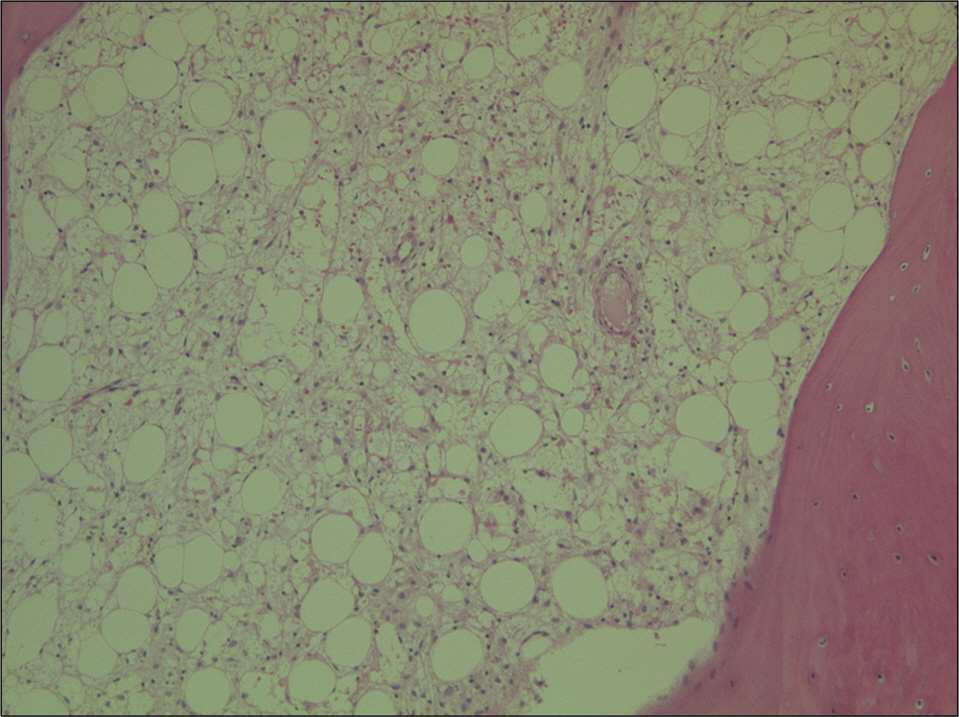
Fig. 2. Bone marrow biopsy of a 3-year-old boy suffered from aplastic anemia after liver transplantation due to fulminant hepatic failure. The cellularity is 0∼10% which is hypocellular with marked decrease of Trilineage hematopoiesis.
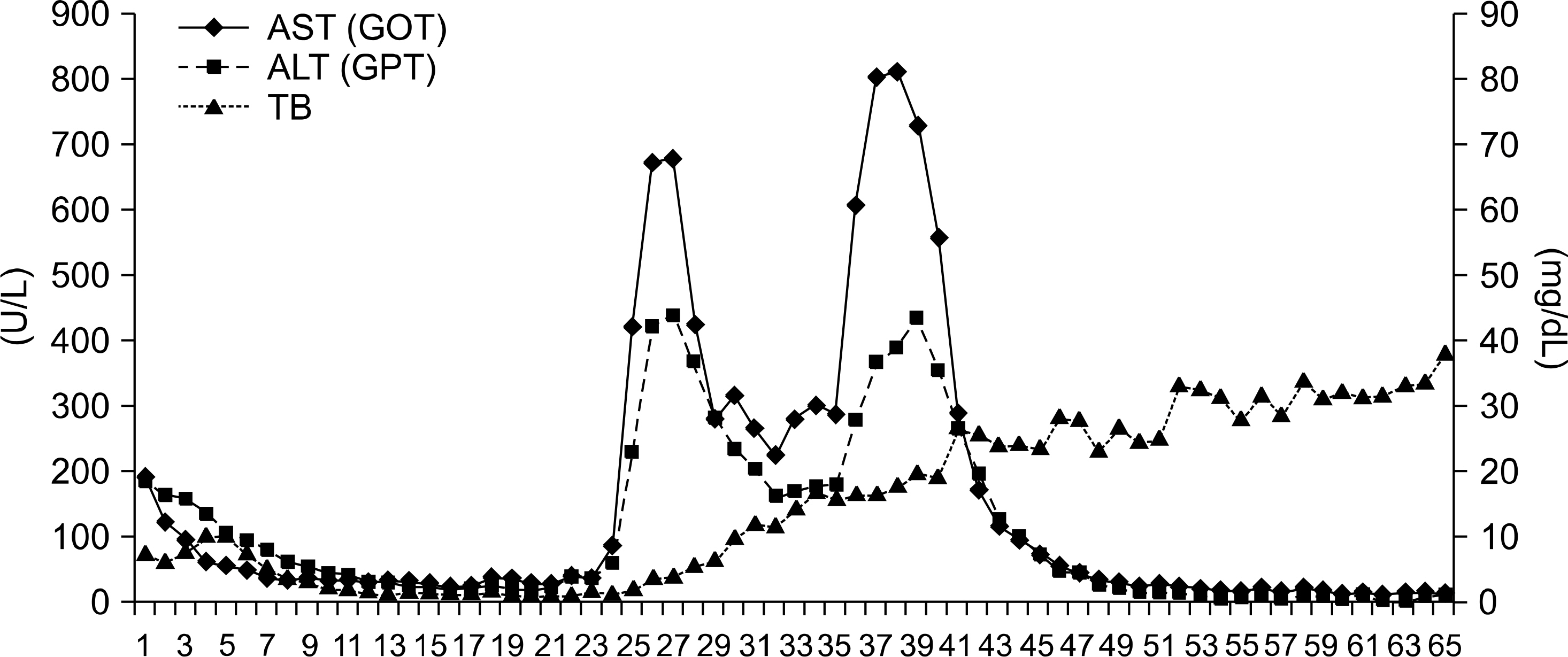
Fig. 3. Plotting of liver function test in a 3-year-old boy after liver transplantation for fulminant hepatic failure. He developed hyperbilirubinemia since 27 days after liver transplantation.
Reference
-
References
1). Misra S, Moore TB, Ament ME, Vargas JH, Busutill RW, McDiarmid SV. Profile of anemia in children after liver transplantation. Transplantation. 2000; 70:1459–63.
Article2). Wintrobe MM. Relation of disease of liver to anemia. Arch Intern Med. 1936; 57:289–306.3). Jarrold T, Vilter RW. Hematologic observations in patients with chronic hepatic insufficiency: sternal bone marrow morphology and bone marrow plasmacytosis. J Clin Invest. 1949; 28:286–92.4). Maruyama S, Hirayama C, Yamamoto S, Kodo M, Udagawa A, Kadowaki Y, et al. Red blood cell status in alcoholic and nonalcoholic liver disease. J Lab Clin Med. 2001; 138:332–7.
Article5). Maheshwari A, Mishra R, Thuluvath PJ. Post-liver-trans-plant anemia: etiology and management. Liver Transpl. 2004; 10:165–73.
Article6). Stock PG, Steiner ME, Freese D, Sharp H, Ascher NL. Hepatitis associated aplastic anemia after liver transplantation. Transplantation. 1987; 43:595–7.7). Kim MJ, Kim I, Bae HM, Seo K, Park N, Yoon SS, et al. Hematopoietic stem cell transplantation after post-transplant lymphoproliferative disorder. J Korean Med Sci. 2010; 25:781–4.
Article8). Ndimbie OK, Frezza E, Jordan JA, Koch W, van Thiel DH. Parvovirus B19 in anemic liver transplant recipients. Clin Diagn Lab Immonol. 1996; 3:756–60.
Article9). Itterbeek P, Vandenberghe P, Nevens F, Fevery J, Aerts R, Yap SH, et al. Aplastic anemia after transplantation for non-A, non-B, non-C fulminant hepatic failure: case re report and view of the literature. Transpl Int. 2002; 15:117–23.10). De Bruyne RM, Dhawan A. Bone marrow dysfunction following pediatric liver transplantation. Pediatr Transplant. 2005; 9:423–6.11). Schrezenmeier H, Bacigalupo A. Aplastic Anemia: Pathophysiology and Treatment. Cambridge, UK: Cambridge University Press;2000. p. 308–15.12). Chong BH. Heparin-induced thrombocytopenia. J Thromb Haemost. 2003; 1:1471–8.
Article13). Hagglund H, Winiarski J, Ringden O, Sparrelid E, Ericzon BG. Successful allogeneic bone marrow transplantation in a 2.5-year-old boy with ongoing cytomegalovirus viremia and severe aplastic anemia after orthotopic liver transplantation for non-A, non-B, non-C hepatitis. Transplantation. 1997; 64:1207–8.
Article14). Dale DC, Liles WC, Price TH. Renewed interest in granulocyte transfusion therapy. Br J Haematol. 1997; 98:497–501.
Article15). Strauss RG. Therapeutic granulocyte transfusions in 1993. Blood. 1993; 81:1675–8.16). Herzig GP, Root RK, Graw RG Jr. Granulocyte collection by continuous flow filtration leukapheresis. Blood. 1972; 39:554–67.17). Higby DJ, Henderson ES, Burnett D, Cohen E. Filtration leukapheresis: effects of donor stimulation with dexamethasone. Blood. 1977; 50:953–9.
Article18). Strauss RG. Clinical perspectives of granulocyte transfusions: efficacy to date. J Clin Apher. 1995; 10:114–8.
Article19). Hubel K, Dale DC, Engert A, Liles WC. Current status of granulocyte (neutrophil) transfusion therapy for infectious diseases. J Infect Dis. 2001; 183:321–8.
Article20). Gonzalez-Casas R, Garcia-Buey L, Jones EA, Gisbert JP, Moreno-Otero R. Systematic review: hepatitis-associated aplastic anaemia-a syndrome associated with abnormal immunological function. Aliment Pharmacol Ther. 2009; 30:436–43.21). Brown KE, Tisdale J, Barrett AJ, Dunbar CE, Young NS. Hepatitis-associated aplastic anemia. N Engl J Med. 1997; 336:1059–64.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Aplastic Anemia following Hepatic Failure by Acute Hepatitis
- Treatment of severe aplastic anemia: comparison between bone marrow transplantation and immunomodulation
- Indication of Pediatric Liver Transplantation
- Post-Hepatitic Aplastic Anemia Associated with Hepatitis A Virus
- Acute Tubulointerstitial Nephritis Induced by Deferasirox following Hematopoietic Stem Cell Transplantation for Severe Aplastic Anemia
