J Korean Med Sci.
2013 Feb;28(2):328-330. 10.3346/jkms.2013.28.2.328.
Extensive Thrombosis in a Patient with Familial Mediterranean Fever, Despite Hyperimmunoglobulin D State in Serum: First Adult Case in Korea
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Inha University Hospital, Incheon, Korea. rhksr@inha.ac.kr
- 2Division of Infectious Disease, Department of Internal Medicine, Inha University Hospital, Incheon, Korea.
- 3Department of General Surgery, Inha University Hospital, Incheon, Korea.
- KMID: 1429215
- DOI: http://doi.org/10.3346/jkms.2013.28.2.328
Abstract
- Familial Mediterranean fever (FMF) is an autosomal recessive disease characterized by recurrent episodes of fever accompanied by peritonitis, pleuritis, arthritis, or erysipelas-like erythema. It is known to occur mainly among Mediterranean and Middle Eastern populations such as non-Ashkenazi Jews, Arabs, Turks, and Armenians. FMF is not familiar to clinicians beyond this area and diagnosing FMF can be challenging. We report a 22-yr old boy who presented with fever, arthalgia and abdominal pain. He had a history of recurrent episodes of fever associated with arthalgia which would subside spontaneously or by antipyretics. Autosomal recessive periodic fever syndromes were suspected. Immunoglobulin D (IgD) level in the serum was elevated and DNA analysis showed complex mutations (p.Glu148Gln, p.Pro369Ser, p.Arg408Gln) in the MEFV gene. 3D angio computed tomography showed total thrombosis of splenic vein with partial thrombosis of proximal superior mesenteric vein, main portal vein and intrahepatic both portal vein. This is a case of FMF associated with multiple venous thrombosis and elevated IgD level. When thrombosis is associated with elevated IgD, FMF should be suspected. This is the first adult case reported in Korea.
Keyword
MeSH Terms
-
Abdominal Pain/etiology
Arthralgia/etiology
Cytoskeletal Proteins/genetics/metabolism
Familial Mediterranean Fever/complications/*diagnosis
Humans
Immunoglobulin D/*blood
Male
Mesenteric Veins
Mevalonate Kinase Deficiency/complications/*diagnosis
Mutation
Portal Vein
Republic of Korea
Splenic Vein
Tomography, X-Ray Computed
Venous Thrombosis/complications/*diagnosis
Young Adult
Cytoskeletal Proteins
Immunoglobulin D
Figure
-
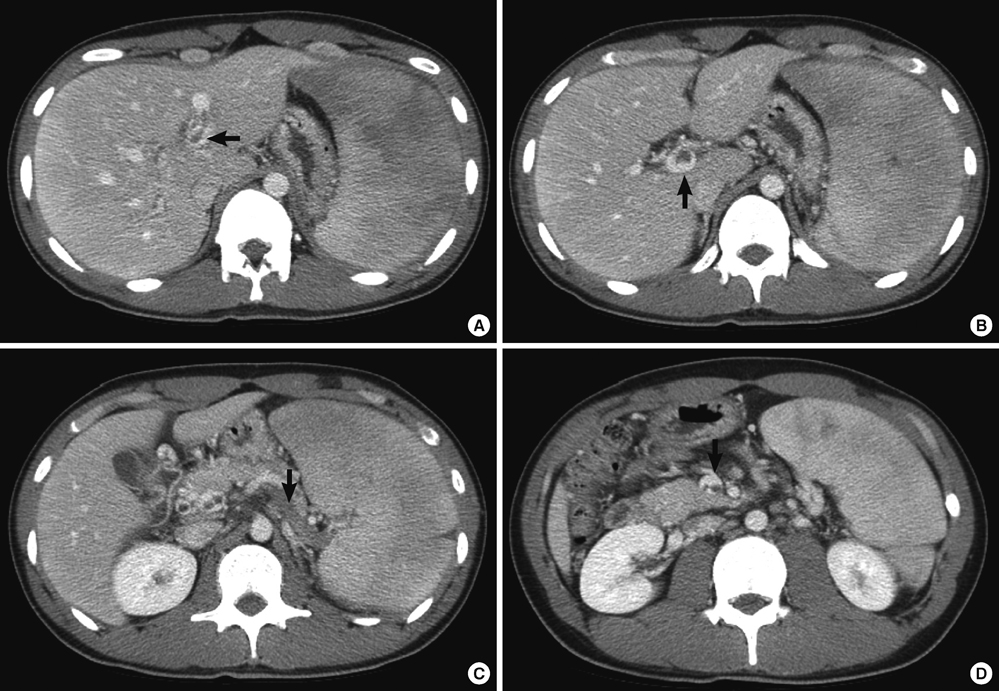
Fig. 1 Serial 3D angio CT scans. Arrows in the CT indicate thrombosis in (A) left portal vein (B) main portal vein (C) splenic vein and (D) superior mesenteric vein.
Cited by 1 articles
-
Familial Mediterranean Fever With Complete Symptomatic Remission During Pregnancy
Kwang Taek Kim, Hyun Joo Jang, Jae Eun Lee, Mi Kang Kim, Jun Jae Yoo, Gye Yeon Lee, Sea Hyub Kae, Jin Lee
Intest Res. 2015;13(3):287-290. doi: 10.5217/ir.2015.13.3.287.
Reference
-
1. Ben-Chetrit E, Levy M. Familial Mediterranean fever. Lancet. 1998. 351:659–664.2. Yamazaki K, Yamazaki T, Masumoto J, Suzuki A, Yazaki M, Agematsu K. Familial Mediterranean fever as representative autoinflammatory disease. Rinsho Byori. 2009. 57:371–381.3. Tsuchiya-Suzuki A, Yazaki M, Nakamura A, Yamazaki K, Agematsu K, Matsuda M, Ikeda S. Clinical and genetic features of familial Mediterranean fever in Japan. J Rheumatol. 2009. 36:1671–1676.4. Koo KY, Park SJ, Wang JY, Shin JI, Jeong HJ, Kim BJ, Lee JS. The first case of Familial Mediterranean Fever associated with renal amyloidosis in Korea. Yonsei Med J. 2012. 53:454–458.5. French Familial Mediterranean Fever Consortium. A candidate gene for familial Mediterranean fever. Nat Genet. 1997. 17:25–31.6. The International Familial Mediterranean Fever Consortium. Ancient missense mutations in a new member of the RoRet gene family are likely to cause familial Mediterranean fever. Cell. 1997. 90:797–807.7. Bernot A, da Silva C, Petit JL, Cruaud C, Caloustian C, Castet V, Ahmed-Arab M, Dross C, Dupont M, Cattan D, et al. Non-founder mutations in the MEFV gene establish this gene as the cause of familial Mediterranean fever (FMF). Hum Mol Genet. 1998. 7:1317–1325.8. Marek-Yagel D, Berkun Y, Padeh S, Abu A, Reznik-Wolf H, Livneh A, Pras M, Pras E. Clinical disease among patients heterozygous for familial Mediterranean fever. Arthritis Rheum. 2009. 60:1862–1866.9. Booty MG, Chae JJ, Masters SL, Remmers EF, Barham B, Le JM, Barron KS, Holland SM, Kastner DL, Aksentijevich I. Familial Mediterranean fever with a single MEFV mutation: Where is the second hit? Arthritis Rheum. 2009. 60:1851–1861.10. Marek-Yagel D, Berkun Y, Padeh S, Abu A, Reznik-Wolf H, Livneh A, Pras M, Pras E. Clinical disease among patients heterozygous for familial Mediterranean fever. Arthritis Rheum. 2009. 60:1862–1866.11. Tchernitchko D, Legendre M, Cazeneuve C, Delahaye A, Niel F, Amselem S. The E148Q MEFV allele is not implicated in the development of familial Mediterranean fever. Hum Mutat. 2003. 22:339–340.12. Topaloglu R, Ozaltin F, Yilmaz E, Ozen S, Balci B, Besbas N, Bakkaloglu A. E148Q is a disease-causing MEFV mutation: a phenotypic evaluation in patients with familial Mediterranean fever. Ann Rheum Dis. 2005. 64:750–752.13. Touitou I. The spectrum of familial Mediterranean fever mutations. Eur J Hum Genet. 2001. 9:473–483.14. Drenth JP, Haagsma CJ, vanderMeer JW. International Hyper-IgD Study Group. Hyperimmunoglobulinemia D and periodic fever syndrome. The clinical spectrum in a series of 50 patients. Medicine (Baltimore). 1994. 73:133–144.15. Medlej-Hashim M, Petit I, Adib S, Chouery E, Salem N, Delague V, Rawashdeh M, Mansour I, Lefranc G, Naman R, et al. Familial Mediterranean fever: association of elevated IgD plasma levels with specific MEFV mutations. Eur J Hum Genet. 2001. 9:849–854.16. Aksu G, Ozturk C, Kavakli K, Genel F, Kutukculer N. Hypercoagulability: interaction between inflammation and coagulation in familial Mediterranean fever. Clin Rheumatol. 2007. 26:366–370.17. Ruiz XD, Gadea CM. Familial Mediterranean fever presenting with pulmonary embolism. Conn Med. 2011. 75:17–19.18. Standing AS, Eleftheriou D, Lachmann HJ, Brogan PA. Familial Mediterranean fever caused by homozygous E148Q mutation complicated by Budd-Chiari syndrome and polyarteritis nodosa. Rheumatology. 2011. 50:624–626.19. Kwon SR, Lim MJ, Park SG, Moon YS, Park W. Decreased protein S activity is related to the disease activity of Behcet's disease. Rheumatol Int. 2006. 27:39–43.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Familial Mediterranean Fever With Complete Symptomatic Remission During Pregnancy
- Familial Mediterranean fever presenting as fever of unknown origin in Korea
- The First Case of Familial Mediterranean Fever Associated with Renal Amyloidosis in Korea
- Familial Mediterranean Fever: The First Adult Case in Korea
- Bloody Diarrhea as a Presentation Manifestation of Familial Mediterranean Fever in a Patient with Compound Heterozygote Mutations of the MEFV Gene
