Application of Ganz Surgical Hip Dislocation Approach in Pediatric Hip Diseases
- Affiliations
-
- 1Department of Orthopaedic Surgery, Seoul National University College of Medicine, Seoul, Korea. tjcho@snu.ac.kr
- 2Department of Orthopaedic Surgery, Jeju National University College of Medicine, Jeju, Korea.
- KMID: 999391
- DOI: http://doi.org/10.4055/cios.2009.1.3.132
Abstract
- BACKGROUND
Ganz surgical hip dislocation is useful in the management of severe hip diseases, providing an unobstructed view of the femoral head and acetabulum. We present our early experience with this approach in pediatric hip diseases. METHODS: Twenty-three hips of 21 patients with pediatric hip diseases treated using the Ganz surgical hip dislocation approach were the subjects of this study. The average age at the time of surgery was 15.7 years. There were 15 male and 6 female patients who were followed for an average of 15.1 months (range, 6 to 29 months). Diagnoses included hereditary multiple exostoses in 9 hips, slipped capital femoral epiphysis in 7, Legg-Calve-Perthes disease in 4, osteoid osteoma in 1, pigmented villonodular synovitis in 1, and neonatal septic hip sequelae in 1. Medical records were reviewed to record diagnoses, principal surgical procedures, operative time, blood loss, postoperative rehabilitation, changes in the range of hip joint motion, and complications. RESULTS: Femoral head-neck osteochondroplasty was performed in 17 patients, proximal femoral realignment osteotomy in 6, open reduction and subcapital osteotomy for slipped capital femoral epiphysis (SCFE) in 2, core decompression and bone grafting in 2, hip distraction arthroplasty in 2, and synovectomy in 2. Operative time averaged 168.6 minutes when only osteochondroplasty and/or synovectomy were performed. Hip flexion range improved from a preoperative mean of 84.7degrees to a mean of 115.0degrees at the latest follow-up visit. Early continuous passive motion and ambulation were stressed in rehabilitation. No avascular necrosis of the femoral head was noted up to the time of the latest follow-up visit, except for in one SCFE patient whose surgical intervention was delayed for medical reasons. CONCLUSIONS: Ganz surgical hip dislocation provides wide exposure of the femoral head and neck, which enables complete and precise evaluation of the femoral head and neck contour. Hence, the extensive impinging bump can be excised meticulously, and the circulation of the femoral head can be monitored during surgery. The Ganz procedure was useful in severe pediatric hip diseases and allowed for quick rehabilitation with fewer complications.
MeSH Terms
Figure
-
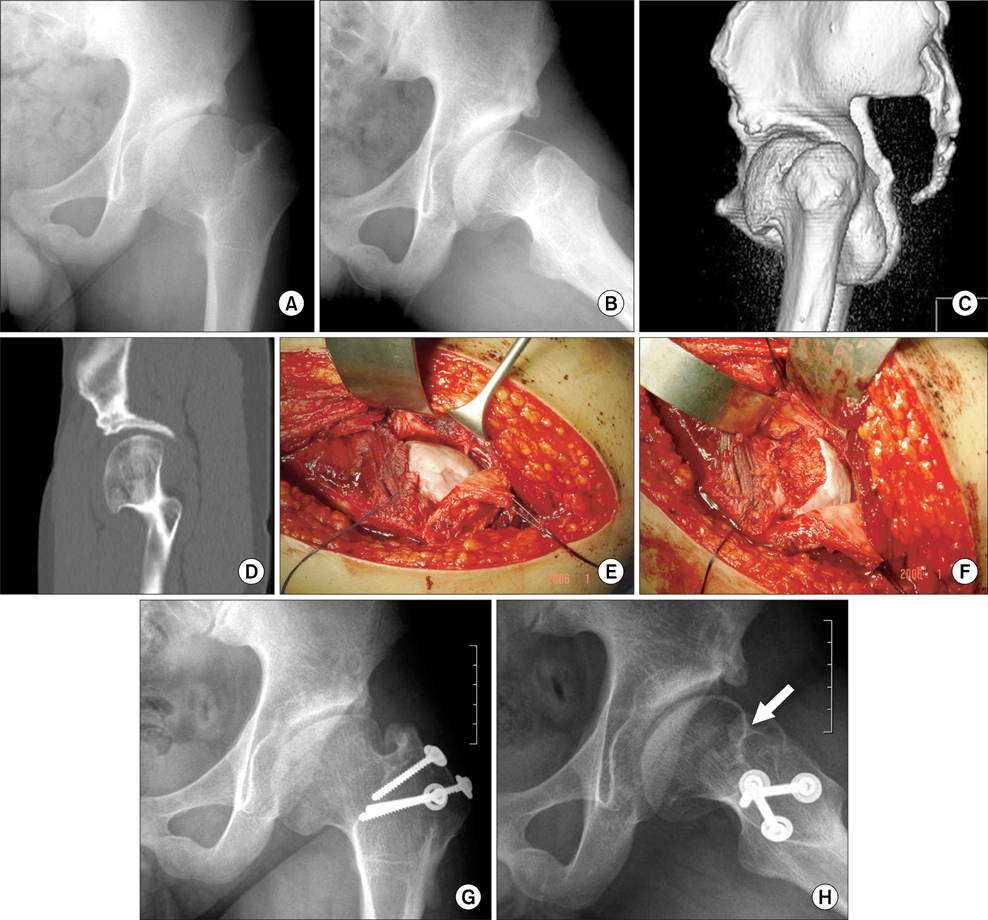
Fig. 1 A 16-year-old boy with Legg-Calvé-Perthes disease of the left hip was treated with femoral valgization osteotomy 6 years ago and shelf acetabuloplasty 3 years ago. He had limited left hip flexion and a positive impingement test (A). Lauenstein view (B), 3D-CT (C), and sagittal reconstruction view (D) revealed an anterior hump of the femoral head causing cam-type femoroacetabular impingement, which was also confirmed in the subluxated femoral head using the Ganz surgical hip dislocation approach (E). Osteochondroplasty relieved the impingement (F). Plain radiographs taken 1.5 years later showed a well-formed head-neck offset (white arrow) (G, H). Hip flexion range improved from 95° in the preoperative period to 130° at 1.5 years follow-up.
Cited by 1 articles
-
Anterolateral Approach in the Treatment of Femoroacetabular Impingement of the Hip
Hui Taek Kim, Um Ji Kim, Yoon Je Cho
Clin Orthop Surg. 2019;11(3):337-343. doi: 10.4055/cios.2019.11.3.337.
Reference
-
1. Ganz R, Gill TJ, Gautier E, Ganz K, Krugel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001. 83(8):1119–1124.2. Lavigne M, Parvizi J, Beck M, Siebenrock KA, Ganz R, Leunig M. Anterior femoroacetabular impingement: part I. Techniques of joint preserving surgery. Clin Orthop Relat Res. 2004. (418):61–66.3. Spencer S, Millis MB, Kim YJ. Early results of treatment of hip impingement syndrome in slipped capital femoral epiphysis and pistol grip deformity of the femoral head-neck junction using the surgical dislocation technique. J Pediatr Orthop. 2006. 26(3):281–285.
Article4. Leunig M, Slongo T, Ganz R. Subcapital realignment in slipped capital femoral epiphysis: surgical hip dislocation and trimming of the stable trochanter to protect the perfusion of the epiphysis. Instr Course Lect. 2008. 57:499–507.5. Philippon MJ, Schenker ML. Arthroscopy for the treatment of femoroacetabular impingement in the athlete. Clin Sports Med. 2006. 25(2):299–308.
Article6. Krueger A, Leunig M, Siebenrock KA, Beck M. Hip arthros copy after previous surgical hip dislocation for femoroacetabular impingement. Arthroscopy. 2007. 23(12):1285–1289.7. Gautier E, Ganz K, Krugel N, Gill T, Ganz R. Anatomy of the medial femoral circumflex artery and its surgical implications. J Bone Joint Surg Br. 2000. 82(5):679–683.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Modified Posterior Approach to Total Hip Arthroplasty
- Posterior Approach to Total Hip Joint Replacement Arthroplasty
- Surgical Treatment of Pathological Dislocation of Child Hip After Acute Osteomyelitis of Ilium
- Anterolateral Approach in the Treatment of Femoroacetabular Impingement of the Hip
- Anterior Approaches in Hip Surgery
