Anterolateral Approach in the Treatment of Femoroacetabular Impingement of the Hip
- Affiliations
-
- 1Department of Orthopedic Surgery, Pediatric Orthopedics and Biomedical Research Institute, Pusan National University Hospital, Busan, Korea. kimht@pusan.ac.kr
- KMID: 2462564
- DOI: http://doi.org/10.4055/cios.2019.11.3.337
Abstract
- BACKGROUND
Ganz surgical hip dislocation via a posterior (Kocher-Langenbeck) approach is a popular procedure in the management of femoroacetabular impingement (FAI). We report the results of surgery performed through an anterolateral (Watson-Jones) approach in the management of anterolateral FAI.
METHODS
Twenty-one hips in 20 patients (mean age at the time of operation, 17.3 years) were treated surgically using an anterolateral approach: 12 hips with Legg-Calvé-Perthes disease, three septic hips, three hips with avascular necrosis (combined with slipped capital femoral epiphysis [SCFE], femoral neck fracture, and developmental dislocation of the hip), two hips with epiphyseal dysplasia, and one hip with SCFE. All patients had anterolateral FAI. Surgical hip dislocation was performed in four hips with trochanteric osteotomy. Combined osteotomies were for neck lengthening in 11 hips, varus or valgus osteotomy in the proximal femur in four hips, and pelvic osteotomy in four hips. Clinical results were evaluated using a modified Harris hip score (mHHS).
RESULTS
Range of hip flexion and abduction showed statistically significant improvement after surgery; however, the improvement in mean mHHS was not statistically significant.
CONCLUSIONS
An anterolateral approach can be used as an alternative to a posterior approach in the management of anterolateral FAI with or without hip dislocation while safely preserving the blood supply to the femoral head and allowing simultaneous procedures in the proximal femur.
MeSH Terms
Figure
-
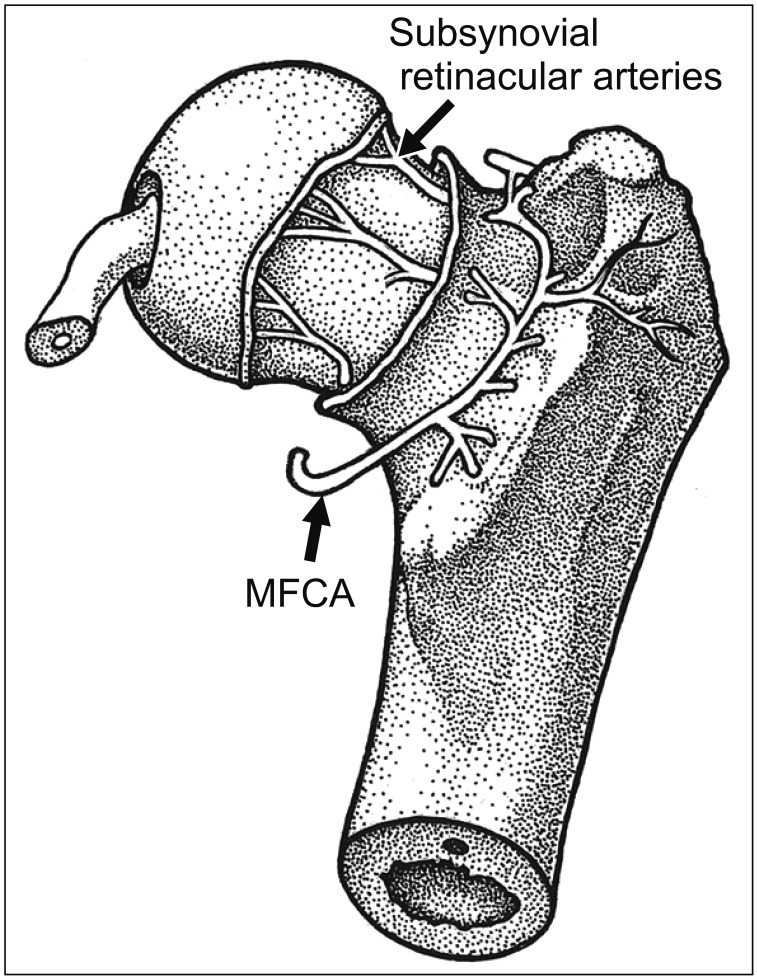
Fig. 1 Arteries of the femoral head and neck viewed from a posterior aspect (surrounding muscles are removed). Subsynovial retinacular arteries enter the capsule from the medial femoral circumflex artery (MFCA). Subperiosteal stripping from the lateral aspect of the femur to the medial side (proximally from the level of the lesser trochanter) and a careful cut of the short external rotators along the bony cortex prevent vascular damage during hip dislocation and simultaneous proximal femoral osteotomy.
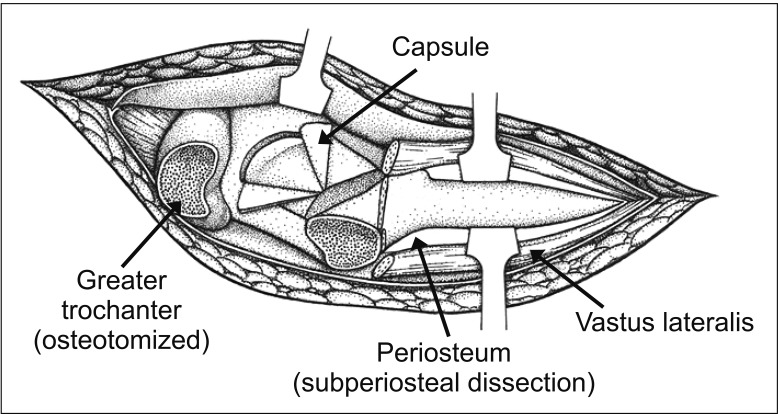
Fig. 2 Illustration of the hip joint and femur before dislocation of the femoral head and osteotomy in the proximal femur showing an osteotomized greater trochanter, opened capsule, longitudinally split vastus lateralis, and subperiosteal dissection to protect the medial femoral circumflex artery.
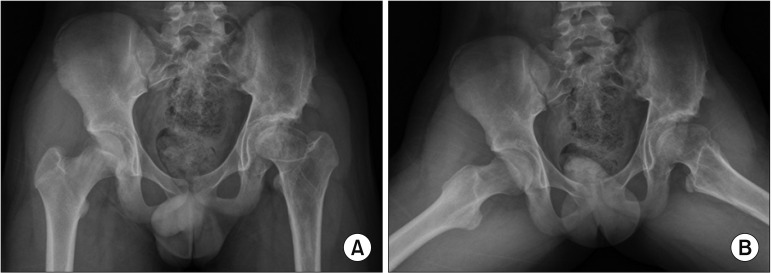
Fig. 3 Anteroposterior (A) and frog-leg lateral (B) views of a 14-year-old boy with Legg-Calvé-Perthes disease in the left hip show a short femoral neck, overgrown greater trochanter, and a 2-cm leg length discrepancy. At age 9 years, he underwent a valgus-flexion femoral osteotomy and then Chiari pelvic osteotomy due to the laterally uncovered femoral head. Clinically he showed limping and limited range of motion, especially in abduction.
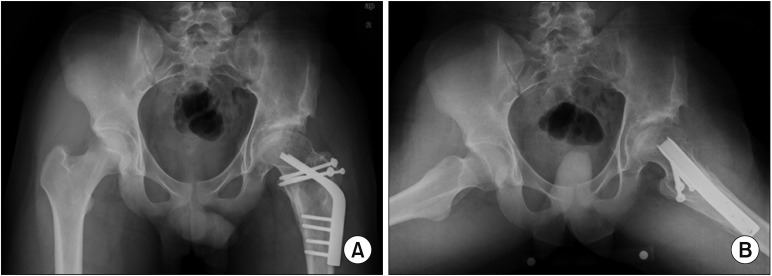
Fig. 4 A patient underwent a neck lengthening osteotomy with lateral and distal transfer of the greater trochanter performed through an anterolateral approach. Simultaneous osteochondroplasty of the anterolateral aspect of the femoral head and neck was also performed through the same approach. Anteroposterior (A) and frog-leg lateral (B) views taken 3 years after surgery (at age 17) show improved biomechanical anatomy of the hip.
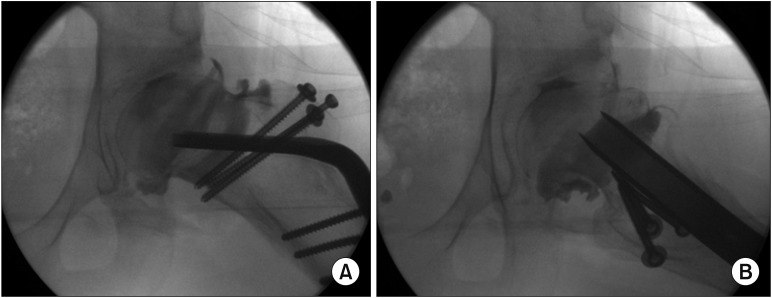
Fig. 5 Abduction (A) and lateral (B) arthrographs show improved sphericity of the femoral head. The hip range of motion improved by 10° in flexion and 15° in abduction.
Cited by 1 articles
-
Corrigendum to “Anterolateral Approach in the Treatment of Femoroacetabular Impingement of the Hip”
Hui Taek Kim, Um Ji Kim, Yoon Jae Cho
Clin Orthop Surg. 2019;11(4):500-500. doi: 10.4055/cios.2019.11.4.500.
Reference
-
1. Ganz R, Gill TJ, Gautier E, Ganz K, Krugel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001; 83(8):1119–1124. PMID: 11764423.2. Gibson A. Posterior exposure of the hip joint. J Bone Joint Surg Br. 1950; 32(2):183–186. PMID: 15422015.
Article3. Letournel E, Judet R. Fractures of the Acetabulum. 2nd ed. Berlin: Springer Verlag;1993. p. 364–369.4. Gautier E, Ganz K, Krugel N, Gill T, Ganz R. Anatomy of the medial femoral circumflex artery and its surgical implications. J Bone Joint Surg Br. 2000; 82(5):679–683. PMID: 10963165.
Article5. Watson-Jones R. Fractures of the neck of the femur. Br J Surg. 1936; 23(92):787–808.
Article6. Buess P, Morscher E. Osteotomy to lengthen the femur neck with distal adjustment of the trochanter major in coxa vara after hip dislocation. Orthopade. 1988; 17(6):485–490. PMID: 3217108.7. Ribas M, Ledesma R, Cardenas C, Marin-Pena O, Toro J, Caceres E. Clinical results after anterior mini-open approach for femoroacetabular impingement in early degenerative stage. Hip Int. 2010; 20 Suppl 7:S36–S42. PMID: 20512770.
Article8. Ng VY, Arora N, Best TM, Pan X, Ellis TJ. Efficacy of surgery for femoroacetabular impingement: a systematic review. Am J Sports Med. 2010; 38(11):2337–2345. PMID: 20489213.9. Parvizi J, Huang R, Diaz-Ledezma C, Og B. Mini-open femoroacetabular osteoplasty: how do these patients do? J Arthroplasty. 2012; 27(8 Suppl):122–125.10. Cohen SB, Huang R, Ciccotti MG, Dodson CC, Parvizi J. Treatment of femoroacetabular impingement in athletes using a mini-direct anterior approach. Am J Sports Med. 2012; 40(7):1620–1627. PMID: 22562788.
Article11. Philippon M, Schenker M, Briggs K, Kuppersmith D. Femoroacetabular impingement in 45 professional athletes: associated pathologies and return to sport following arthroscopic decompression. Knee Surg Sports Traumatol Arthrosc. 2007; 15(7):908–914. PMID: 17479250.
Article12. Byrd JW, Jones KS. Arthroscopic management of femoroacetabular impingement: minimum 2-year follow-up. Arthroscopy. 2011; 27(10):1379–1388. PMID: 21862276.
Article13. Bedi A, Galano G, Walsh C, Kelly BT. Capsular management during hip arthroscopy: from femoroacetabular impingement to instability. Arthroscopy. 2011; 27(12):1720–1731. PMID: 22047925.
Article14. Nho SJ, Magennis EM, Singh CK, Kelly BT. Outcomes after the arthroscopic treatment of femoroacetabular impingement in a mixed group of high-level athletes. Am J Sports Med. 2011; 39 Suppl:14S–19S. PMID: 21709027.
Article15. Alradwan H, Philippon MJ, Farrokhyar F, et al. Return to preinjury activity levels after surgical management of femoroacetabular impingement in athletes. Arthroscopy. 2012; 28(10):1567–1576. PMID: 22795753.
Article16. Malviya A, Stafford GH, Villar RN. Impact of arthroscopy of the hip for femoroacetabular impingement on quality of life at a mean follow-up of 3.2 years. J Bone Joint Surg Br. 2012; 94(4):466–470. PMID: 22434460.
Article17. Beck M, Leunig M, Parvizi J, Boutier V, Wyss D, Ganz R. Anterior femoroacetabular impingement: part II. Mid-term results of surgical treatment. Clin Orthop Relat Res. 2004; (418):67–73.18. Murphy S, Tannast M, Kim YJ, Buly R, Millis MB. Debridement of the adult hip for femoroacetabular impingement: indications and preliminary clinical results. Clin Orthop Relat Res. 2004; (429):178–181.19. Beaule PE, Le Duff MJ, Zaragoza E. Quality of life following femoral head-neck osteochondroplasty for femoroacetabular impingement. J Bone Joint Surg Am. 2007; 89(4):773–779. PMID: 17403799.20. Yun HH, Shon WY, Yun JY. Treatment of femoroacetabular impingement with surgical dislocation. Clin Orthop Surg. 2009; 1(3):146–154. PMID: 19885050.
Article21. Kempthorne JT, Armour PC, Rietveld JA, Hooper GJ. Surgical dislocation of the hip and the management of femoroacetabular impingement: results of the Christchurch experience. ANZ J Surg. 2011; 81(6):446–450. PMID: 22295348.
Article22. Naal FD, Miozzari HH, Wyss TF, Notzli HP. Surgical hip dislocation for the treatment of femoroacetabular impingement in high-level athletes. Am J Sports Med. 2011; 39(3):544–550. PMID: 21173196.
Article23. Papalia R, Del Buono A, Franceschi F, Marinozzi A, Maffulli N, Denaro V. Femoroacetabular impingement syndrome management: arthroscopy or open surgery? Int Orthop. 2012; 36(5):903–914. PMID: 22190060.
Article24. Sink EL, Fabricant PD, Pan Z, Dayton MR, Novais E. Results of treatment of femoroacetabular impingement in adolescents with a surgical hip dislocation approach. Clin Orthop Relat Res. 2013; 471(8):2563–2569. PMID: 23653097.
Article25. Shin SJ, Kwak HS, Cho TJ, et al. Application of Ganz surgical hip dislocation approach in pediatric hip diseases. Clin Orthop Surg. 2009; 1(3):132–137. PMID: 19885048.
Article26. Trueta J, Harrison MH. The normal vascular anatomy of the femoral head in adult man. J Bone Joint Surg Br. 1953; 35(3):442–461. PMID: 13084696.
Article27. Sevitt S, Thompson RG. The distribution and anastomoses of arteries supplying the head and neck of the femur. J Bone Joint Surg Br. 1965; 47(3):560–573. PMID: 14341080.
Article28. McCarthy JC, Noble PC, Schuck MR, Wright J, Lee J. The Otto E. Aufranc Award: the role of labral lesions to development of early degenerative hip disease. Clin Orthop Relat Res. 2001; (393):25–37. PMID: 11764355.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Efficacy of Intra-articular Steroid Injection in Patients with Femoroacetabular Impingement
- Controversial Issues in Arthroscopic Surgery for Femoroacetabular Impingement
- Femoroacetabular Impingement Syndrome
- Arthroscopic Treatment of Femoroacetabular Impingement of the Hip: 5-7 Years Result
- The Etiology of Residual Symptoms after Hip Arthroscopic Treatment of Femoroacetabular Impingement: Analysis Using Finite Element Modeling
