Pulmonary Artery Embolotherapy in a Patient with Type I Hepatopulmonary Syndrome after Liver Transplantation
- Affiliations
-
- 1Department of Surgery, Konkuk University School of Medicine, Seoul 143-729, Korea.
- 2Department of Surgery, Seoul National University College of Medicine, Seoul 110-744, Korea. kssuh@plaza.snu.ac.kr
- 3Department of Radiology, Seoul National University College of Medicine, Seoul 110-744, Korea.
- 4Department of Nuclear Medicine, Seoul National University College of Medicine, Seoul 110-744, Korea.
- KMID: 984905
- DOI: http://doi.org/10.3348/kjr.2010.11.4.485
Abstract
- Although liver transplantation (LT) is the only effective treatment option for hepatopulmonary syndrome (HPS), the post-LT morbidity and mortality have been high for patients with severe HPS. We performed post-LT embolotherapy in a 10-year-old boy who had severe type I HPS preoperatively, but he failed to recover early from his hypoxemic symptoms after an LT. Multiple embolizations were then successfully performed on the major branches that formed the abnormal vascular structures. After the embolotherapy, the patient had symptomatic improvement and he was discharged without complications.
Keyword
MeSH Terms
Figure
-
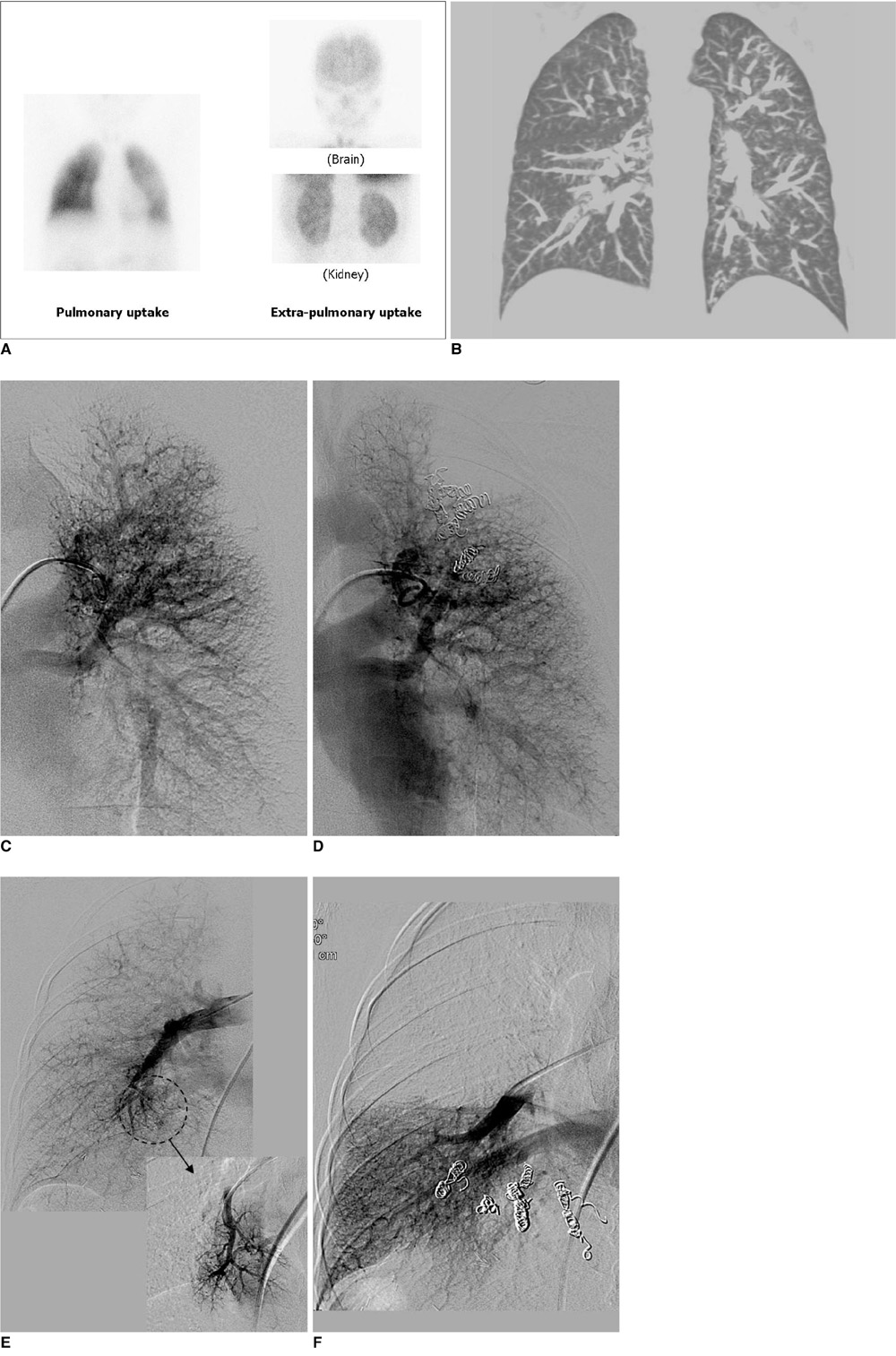
Fig. 1 Embolotherapy for hepatopulmonary syndrome in 10-year-old boy. A. 99m-Tc macroaggregated albumin lung perfusion scanning. Large proportion of radioactive substance was detected in extra-pulmonary areas; mainly brain and kidneys. Amount of intrapulmonary shunting was 45% with assuming that 13% of cardiac output is delivered to brain. B. Pre-transplant pulmonary CT angiography shows diffuse peripheral pulmonary vasodilatation. C. Pre-embolization angiography shows abnormal tortuous and dilated vascular structures in left upper lung field. D. We performed embolization with 8 coils by selecting major branches that formed abnormal vascular structures. Right after embolization, we noted marked decrease in size of abnormal vascular structures and SaO2 had increased by 10%. E. Pre-embolization angiography shows abnormal dilated vascular structures were mainly located in right lower lung field. F. We performed embolization with 9 coils. Patient was discharged three days after second embolization with O2 supplementation of 5 L/min.
Reference
-
1. Swanson KL, Wiesner RH, Krowka MJ. Natural history of hepatopulmonary syndrome: impact of liver transplantation. Hepatology. 2005. 41:1122–1129.2. Mandell MS. The diagnosis and treatment of hepatopulmonary syndrome. Clin Liver Dis. 2006. 10:387–405.3. Palma DT, Fallon MB. The hepatopulmonary syndrome. J Hepatol. 2006. 45:617–625.4. Krowka MJ, Wiseman GA, Burnett OL, Spivey JR, Therneau T, Porayko MK, et al. Hepatopulmonary syndrome: a prospective study of relationships between severity of liver disease, PaO(2) response to 100% oxygen, and brain uptake after (99m)Tc MAA lung scanning. Chest. 2000. 118:615–624.5. Arguedas MR, Fallon MB. Hepatopulmonary syndrome. Clin Liver Dis. 2005. 9:733–746.6. Arguedas MR, Abrams GA, Krowka MJ, Fallon MB. Prospective evaluation of outcomes and predictors of mortality in patients with hepatopulmonary syndrome undergoing liver transplantation. Hepatology. 2003. 37:192–197.7. Lange PA, Stoller JK. The hepatopulmonary syndrome. Effect of liver transplantation. Clin Chest Med. 1996. 17:115–123.8. Poterucha JJ, Krowka MJ, Dickson ER, Cortese DA, Stanson AW, Krom RA. Failure of hepatopulmonary syndrome to resolve after liver transplantation and successful treatment with embolotherapy. Hepatology. 1995. 21:96–100.9. Saad NE, Lee DE, Waldman DL, Saad WE. Pulmonary arterial coil embolization for the management of persistent type I hepatopulmonary syndrome after liver transplantation. J Vasc Interv Radiol. 2007. 18:1576–1580.10. Ryu JK, Oh JH. Hepatopulmonary syndrome: angiography and therapeutic embolization. Clin Imaging. 2003. 27:97–100.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anesthesia for Liver Transplantation in Patients with Hepatopulmonary Syndrome
- Hepatopulmonary Syndrome with Finger Clubbing
- A Case of Hepatopulmonary Syndrome Due to Intrapulmonary Shunting in a Patient with Liver Cirrhosis
- A Case of Hepatopulmonary Syndrome in a Patient with Child-Pugh Class A Liver Cirrhosis
- A case of hepatopulmonary syndrome in a child with fatty liver disease secondary to hypopituitarism after craniopharyngioma resection
