Severe cerebral vasospasm following non-K1 Escherichia coli meningitis: a case report
- Affiliations
-
- 1Department of Neurology, Brown University Health, Providence, Ri, USA
- 2Department of Pathology and Laboratory Medicine, The Warren Alpert Medical School of Brown University, Providence, RI, USA
- 3Division of Infectious Diseases, Warren Alpert Medical School of Brown University, Providence, RI, USA
- 4Department of Diagnostic Imaging, Brown University Health, Providence, RI, USA
- 5Department of Neurology, Warren Alpert Medical School of Brown University, Providence, RI, USA
- KMID: 2563029
- DOI: http://doi.org/10.18700/jnc.240037
Abstract
- Background
Cerebral vasospasm has been reported following various forms of bacterial meningitis; however, there have been no prior reports of meningitis caused by the non-K1 strain of Escherichia coli.
Case Report
A 63-year-old man with chronic thrombocytopenia presented with new-onset seizures that progressed to coma. Cerebrospinal fluid (CSF) analysis showed Gram-negative rods, but CSF culture and the Biofire FilmArray Meningitis/Encephalitis Panel were negative. Additional 16S ribosomal ribonucleic acid (rRNA) polymerase chain reaction and sequencing of the CSF sample indicated E. coli meningitis when correlated with the results of urine culture. The patient eventually developed diffuse cerebral arterial vasospasms with multifocal brain infarcts that progressed to brain death.
Conclusion
E. coli meningitis in adults may be missed if diagnostic tests include only K1 strains. Clinicians should be aware of cerebral vasospasm as a potentially serious complication of E. coli meningitis, and should consider screening for it, particularly in patients with associated risk factors.
Figure
-
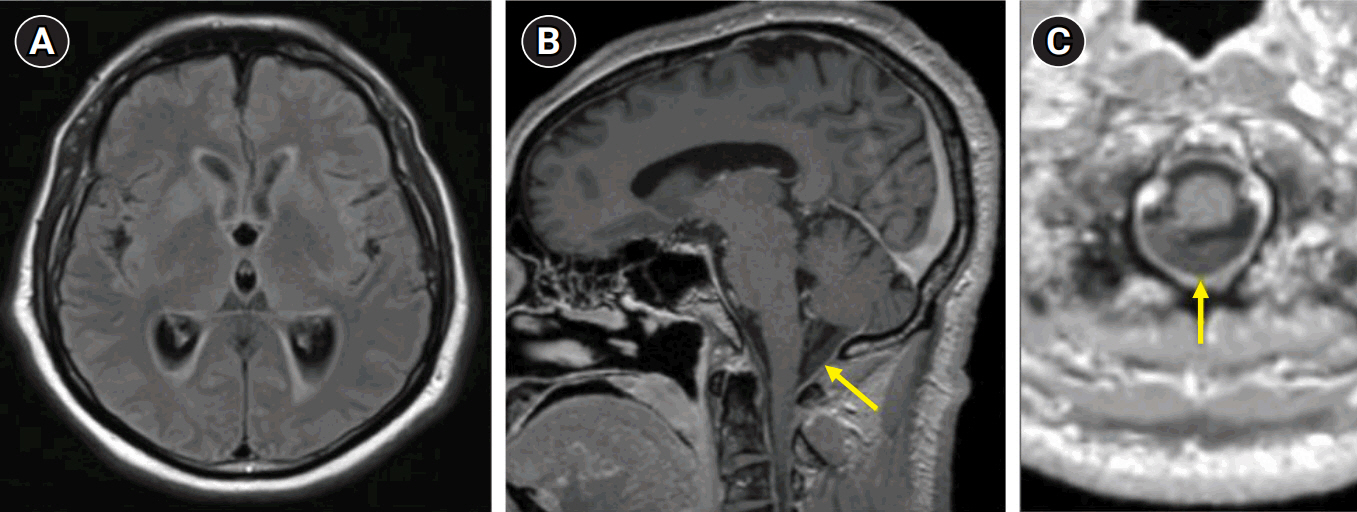
Fig. 1. (A) Axial magnetic resonance image (MRI) of the brain showing a periventricular T2/fluid-attenuated inversion recovery signal consistent with transependymal edema from the acute communicating hydrocephalus. Sagittal (B) and axial (C) T1-weighted post-contrast MRI of the brain with arrows pointing to purulent fluid in the cisterna magna.
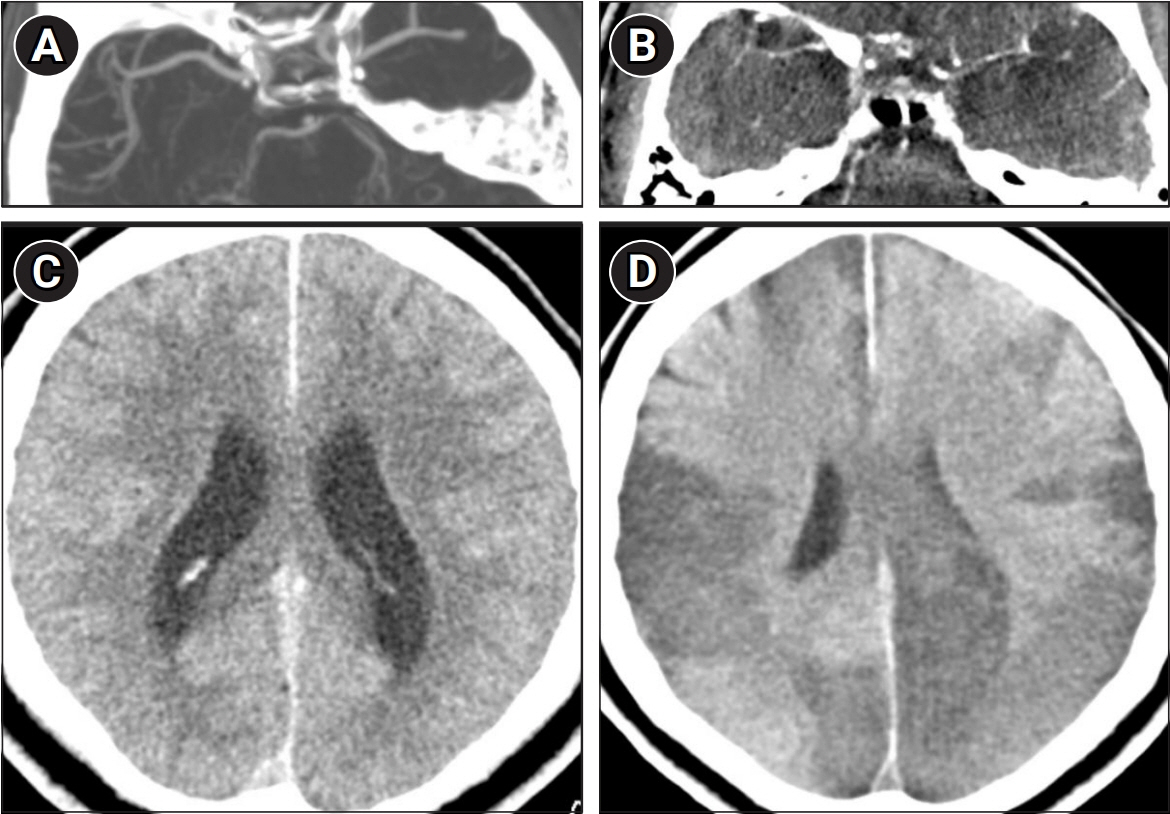
Fig. 2. (A) Axial computed tomography (CT) angiogram, with maximum intensity projection, demonstrating full caliber arteries on hospitalization day 2. (B) Axial contrast enhanced CT showing vasospasm of both the middle cerebral arteries on hospitalization day 8. (C) Axial non-contrast CT prior showing no ischemic burden on hospitalization day 2. (D) Axial non-contrast CT showing multilobar hypodensities consistent with infarction from vasospasm, with associated cerebral edema, on hospitalization day 8.
Reference
-
1. Stoll BJ, Hansen NI, Sánchez PJ, Faix RG, Poindexter BB, Van Meurs KP, et al. Early onset neonatal sepsis: the burden of group B Streptococcal and E. coli disease continues. Pediatrics. 2011; 127:817–26.
Article2. Kim KS. Human meningitis-associated Escherichia coli. EcoSal Plus. 2016; 7:10.1128/ecosalplus.ESP-0015-2015.3. Cabellos C, Verdaguer R, Olmo M, Fernández-Sabé N, Cisnal M, Ariza J, et al. Community-acquired bacterial meningitis in elderly patients: experience over 30 years. Medicine (Baltimore). 2009; 88:115–9.4. Okike IO, Ribeiro S, Ramsay ME, Heath PT, Sharland M, Ladhani SN. Trends in bacterial, mycobacterial, and fungal meningitis in England and Wales 2004-11: an observational study. Lancet Infect Dis. 2014; 14:301–7.
Article5. Bodilsen J, Brouwer MC, Kjærgaard N, Sirks MJ, van der Ende A, Nielsen H, et al. Community-acquired meningitis in adults caused by Escherichia coli in Denmark and The Netherlands. J Infect. 2018; 77:25–9.
Article6. BioFire Diagnostics. FilmArray Meningitis/Encephalitis (ME) Panel CE-IVD Instruction Booklet (RFIT-PRT-0005). BioFire Diagnostics; 2015.7. Schut ES, Brouwer MC, de Gans J, Florquin S, Troost D, van de Beek D. Delayed cerebral thrombosis after initial good recovery from pneumococcal meningitis. Neurology. 2009; 73:1988–95.
Article8. Klein M, Koedel U, Pfefferkorn T, Zeller G, Woehrl B, Pfister HW. Arterial cerebrovascular complications in 94 adults with acute bacterial meningitis. Crit Care. 2011; 15:R281.
Article9. Benadji A, Debroucker T, Martin-Blondel G, Argaud L, Vitrat V, Biron C, et al. Cerebrovascular complications in patients with community-acquired bacterial meningitis: occurrence and associated factors in the COMBAT multicenter prospective cohort. BMC Infect Dis. 2023; 23:376.
Article10. Gogia B, Young AL, O’Brien BJ, Okhuysen PC, Kumar VA. Bihemispheric cortical infarcts in an adult secondary to Escherichia coli K1 meningitis. Case Rep Neurol. 2021; 13:572–7.
Article11. Batino LK, Cinco MT, Navarro JC, Badillo SP, Qureshi AI, Sharma VK. Transcranial Doppler ultrasonography in bacterial meningitis: a systematic review. J Clin Ultrasound. 2024; 52:78–85.
Article12. Norman S, Rosenberg J, Sundararajan SH, Al Balushi A, Boddu SR, Ch’ang JH. Management of refractory bacterial meningitis-associated cerebral vasospasm: illustrative case. J Neurosurg Case Lessons. 2023; 5:CASE22418.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Interaction of Escherichia coli K1 and K5 with Acanthamoeba castellanii Trophozoites and Cysts
- A Case of Subdural Empyema Caused by Escherichia coli Infection
- Effects of Topiramate on the Brain Cell Energy Metabolism in the Early Phase of Experimental Escherichia coli Meningitis
- Escherichia coli O157: H7 Infection
- Effects of decreased cerebral perfusion pressure on cerebral hemodynamics, brain cell membrane function and energy metabolism during the early phase of experimental Escherichia coli meningitis in the newborn piglet
