Clinicopathological and endoscopic features of Helicobacter pylori infection-negative gastric cancer in Japan: a retrospective study
- Affiliations
-
- 1Department of Endoscopy, Fukuoka University Chikushi Hospital, Fukuoka, Japan
- 2Department of Pathology, Fukuoka University Chikushi Hospital, Fukuoka, Japan
- 3Department of Gastroenterology, Fukuoka University Chikushi Hospital, Fukuoka, Japan
- KMID: 2558105
- DOI: http://doi.org/10.5946/ce.2023.258
Abstract
- Background/Aims
Helicobacter pylori infection-negative gastric cancer (HPNGC) has not been systematically investigated in consecutive patients. Hence, this study aimed to investigate the clinicopathological and endoscopic features of HPNGC.
Methods
This single-center retrospective study selected participants from patients with gastric cancer who were treated at the Fukuoka University Chikushi Hospital between January 2013 and December 2021. Only patients diagnosed with HPNGC were enrolled, and their clinicopathological and endoscopic features were analyzed in detail.
Results
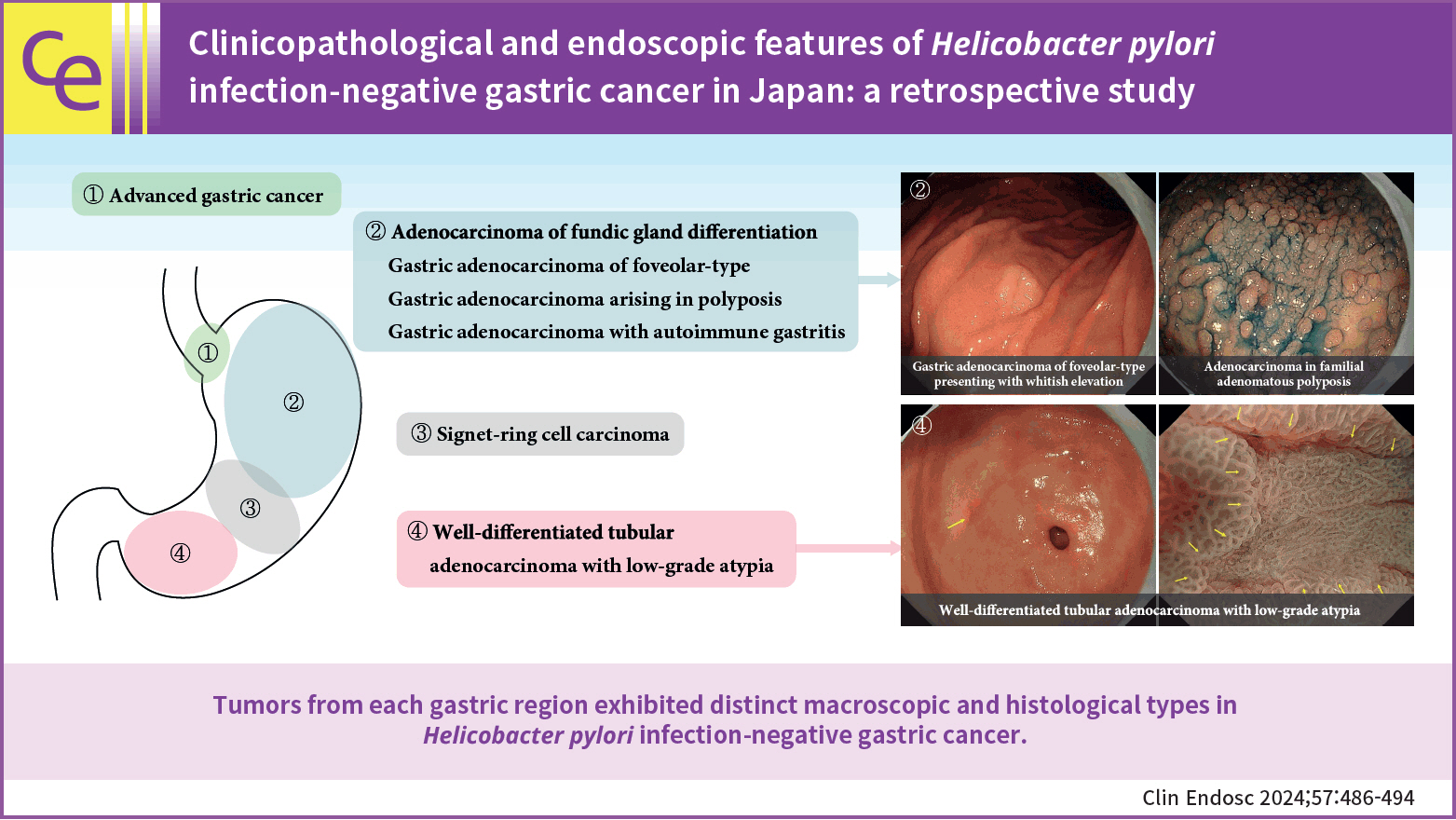
The prevalence of HPNGC in the present study was 2.6% (54/2112). The types of HPNGC observed in each gastric region were as follows: advanced gastric cancer was observed in the cardia; gastric adenocarcinoma of fundic-gland differentiation, gastric adenocarcinoma of foveolar-type presenting with whitish elevation and raspberry-like foveolar-type gastric adenocarcinoma, gastric adenocarcinoma arising in polyposis, and gastric adenocarcinoma with autoimmune gastritis were observed in the fundic gland region ranging from the gastric fornix to the gastric body; signet-ring cell carcinoma was observed in the gastric-pyloric transition region ranging from the lower gastric body to the gastric angle; and well-differentiated tubular adenocarcinoma with low-grade atypia was observed in the antrum.
Conclusions
This study revealed that tumors from each gastric region exhibited distinct macroscopic and histological types in HPNGC.
Figure
-
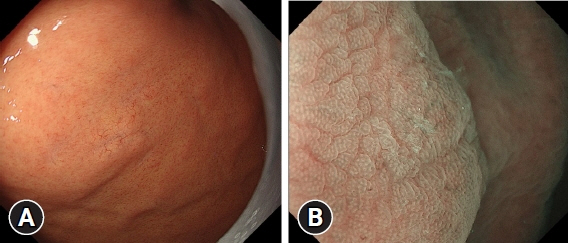
Fig. 1. Endoscopic findings of gastric adenocarcinoma of fundic-gland type. (A) Conventional endoscopic image: a pale subepithelial tumor-like elevated lesion is observed in the fundus. Dilated vessels can be seen in the elevated region. (B) Image of the lesion obtained using magnifying endoscopy with narrow-band imaging. Upon observing the surrounding area, the lesion shows no marked changes in the microvascular (MV) or microsurface (MS) pattern, and there is no clear demarcation line (DL). The microvessel has a polygonal closed-loop morphology, and the vessels are uniform in shape, arranged regularly, and symmetrically distributed. The marginal crypt epithelium has an oval or arc-shaped morphology, is uniform in shape, arranged regularly, and distributed symmetrically. According to the vessel plus surface classification system, the lesion is classified as having a regular MV pattern plus a regular MS pattern without DL. In other words, the magnifying endoscopic findings of the lesion does not fulfill the diagnostic criteria for cancer.
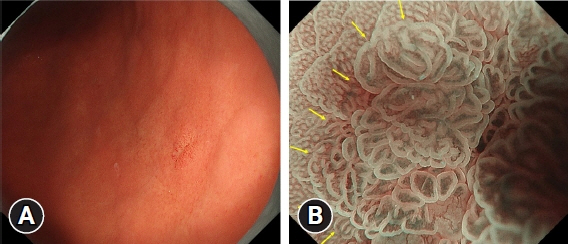
Fig. 2. Endoscopic findings of gastric adenocarcinoma of fundic-gland mucosa type. (A) Conventional endoscopic image. The lesion has a slightly red mucosa in the posterior wall of the lower gastric body. (B) Image of the lesion obtained using magnifying endoscopy with narrow-band imaging. Upon observing the background mucosa, the elevated lesion shows marked changes in both the microvascular (MV) and microsurface (MS) patterns, and there is a clear demarcation line (DL) (yellow arrows). Regarding the MV pattern, the lesion consists of microvessels with open- and closed-loop formation, and the vessels are not uniform in shape, distributed asymmetrically, and arranged irregularly. Regarding the MS pattern, the marginal crypt epithelium (MCE) has a curved or oval morphology. The MCE is nonuniform in shape, distributed asymmetrically, and arranged irregularly. According to the vessel plus surface classification system, the lesion was classified as having an irregular MV pattern plus an irregular MS pattern with a DL, and was diagnosed as cancer.
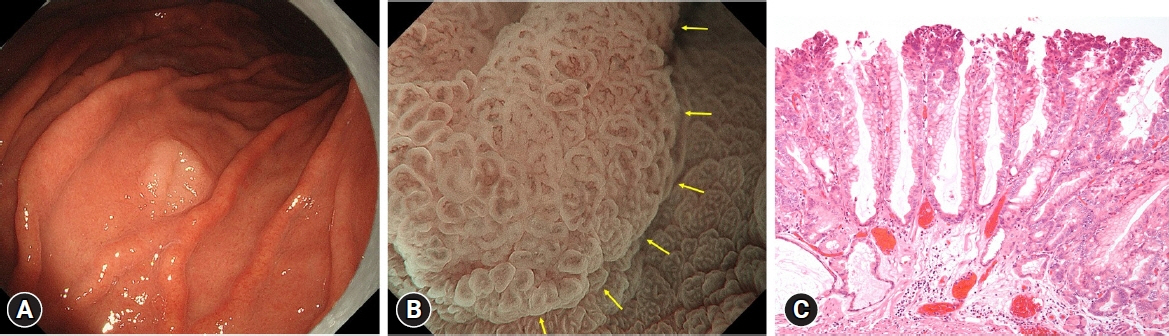
Fig. 3. Endoscopic and histopathological findings of gastric adenocarcinoma of foveolar-type presenting with whitish elevation. (A) Conventional endoscopic findings. A markedly whitish elevated lesion is observed in the greater curvature of the upper gastric body. (B) Image of the lesion obtained using magnifying endoscopy with narrow-band imaging. Upon observation of the background mucosa, the lesion shows marked changes both in microvascular (MV) and microsurface (MS) patterns, and there is a clear demarcation line (DL) (yellow arrows). With respect to the MV pattern, the lesion consists of microvessels with open- and closed-loop formation, and the vessels are not uniform in shape, distributed asymmetrically, and arranged irregularly. With respect to the MS pattern, the marginal crypt epithelium (MCE) has a curved or oval morphology. The MCE is nonuniform in shape, distributed asymmetrically, and arranged irregularly. According to the vessel plus surface classification system, the lesion was classified as having an irregular MV pattern plus an irregular MS pattern with a DL, and was diagnosed as cancer. (C) Histopathological image of gastric adenocarcinoma of foveolar-type presenting with whitish elevation (hematoxylin and eosin stain, ×100). Tall cells with clear cytoplasm are proliferating in a papillary pattern. They exhibit histopathological features of foveolar-type gastric adenocarcinoma.

Fig. 4. Endoscopic and histopathological findings of adenocarcinoma in familial adenomatous polyposis. (A) Conventional endoscopic image. Multiple fundic gland polyps can be seen developing in a region ranging from the gastric fornix to the gastric body. A whitish area is observed in the greater curvature of the upper gastric body. (B) Imaging result of indigocarmine staining. The whitish area appears to have a smaller granular elevation than the surrounding area. (C) Image of the lesion obtained using magnifying endoscopy with narrow-band imaging. Upon observation of the background mucosa, the lesion shows marked changes both in the microvascular (MV) and microsurface (MS) patterns, and there is a clear demarcation line (DL) (yellow arrows). With respect to the MV pattern, the lesion consists of microvessels with open- and closed- loop formation, and the vessels are not uniform in shape, distributed asymmetrically, and arranged irregularly. With respect to the MS pattern, almost no marginal crypt epithelium can be visualized. According to the vessel pulse surface classification system, the lesion was classified as having an irregular MV pattern plus an absent MS pattern with a DL, and was diagnosed as cancer. (D) Histopathological image of adenocarcinoma in familial adenomatous polyposis (hematoxylin and eosin stain, ×40). The histological findings of well-differentiated tubular adenocarcinoma are observed (red line). The mucosa surrounding the tumor exhibits the findings of fundic gland polyps with fundic gland hyperplasia and cyst formation (blue line).

Fig. 5. Endoscopic and histopathological findings of well-differentiated adenocarcinoma with low-grade atypia. (A) Conventional endoscopic image. There are multiple small red depressed lesions in the antrum. The yellow arrow indicates the lesion. (B) Image of the lesion obtained using magnifying endoscopy with narrow-band imaging. The lesion shows marked changes in both microvascular (MV) and microsurface (MS) patterns, with a clear demarcation line (DL) (yellow arrows). With respect to the MV pattern, the lesion mainly consists of microvessels with open-loop formation, and the vessels are not uniform in shape, distributed asymmetrically, and arranged irregularly. With respect to the MS pattern, the marginal crypt epithelium (MCE) has a curved morphology. The MCE is nonuniform in shape, distributed asymmetrically, and arranged irregularly. According to the vessel plus surface classification system, the lesion was classified as having an irregular MV pattern plus an irregular MS pattern with a DL, and was diagnosed as cancer. (C) Histopathological appearance (hematoxylin and eosin stain, ×40). The tumor shows slightly irregular branching ducts with mildly enlarged nuclei and is diagnosed as a well-differentiated adenocarcinoma with low-grade atypia (red arrow). (D) Histopathological findings in the background mucosa of the lesion (hematoxylin and eosin stain, ×40). Gastric intestinal metaplasia is observed.
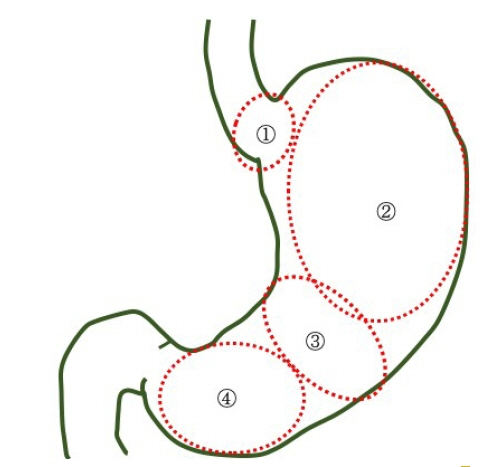
Fig. 6. Characteristics of the preferential development sites of Helicobacter pylori infection-negative gastric cancer. (1) Cardia: advanced gastric cancer. (2) Fundic gland region ranging from the gastric fornix to the gastric body: adenocarcinoma of fundic gland differentiation (adenocarcinoma of fundic-gland type, adenocarcinoma of fundic-gland mucosa type, adenocarcinoma of mixed fundic and pyloric-mucosa types), gastric adenocarcinoma of foveolar-type (gastric adenocarcinoma of foveolar-type presenting with whitish elevation, raspberry-like foveolar-type gastric adenocarcinoma), gastric adenocarcinoma arising in polyposis (adenocarcinoma in Peutz-Jeghers syndrome, adenocarcinoma in familial adenomatous polyposis), and gastric adenocarcinoma with autoimmune gastritis. (3) Gastric-pyloric transition region ranging from the lower gastric body to the gastric angle: signet-ring cell carcinoma. (4) Antrum: well-differentiated adenocarcinoma with low-grade atypia.
Cited by 1 articles
-
Is your endoscopist qualified enough to detect
Helicobacter pylori -naive status?
Sun-Young Lee
Clin Endosc. 2024;57(4):466-467. doi: 10.5946/ce.2024.033.
Reference
-
1. Warren JR, Marshall B. Unidentified curved bacilli on gastric epithelium in active chronic gastritis. Lancet. 1983; 1:1273–1275.2. Infection with Helicobacter pylori. IARC Monogr Eval Carcinog Risks Hum. 1994; 61:177–240.3. Kamada T, Haruma K, Ito M, et al. Time trends in Helicobacter pylori infection and atrophic gastritis over 40 years in Japan. Helicobacter. 2015; 20:192–198.4. Ono S, Kato M, Suzuki M, et al. Frequency of Helicobacter pylori -negative gastric cancer and gastric mucosal atrophy in a Japanese endoscopic submucosal dissection series including histological, endoscopic and serological atrophy. Digestion. 2012; 86:59–65.
Article5. Kim HJ, Kim N, Yoon H, et al. Comparison between resectable Helicobacter pylori-negative and -positive gastric cancers. Gut Liver. 2016; 10:212–219.
Article6. Yamada A, Kaise M, Inoshita N, et al. Characterization of Helicobacter pylori-naïve early gastric cancers. Digestion. 2018; 98:127–134.
Article7. Sato C, Hirasawa K, Tateishi Y, et al. Clinicopathological features of early gastric cancers arising in Helicobacter pylori uninfected patients. World J Gastroenterol. 2020; 26:2618–2631.
Article8. Akazawa Y, Ueyama H, Hayashi T, et al. Clinicopathological and molecular characterization of early gastric adenocarcinoma in Helicobacter pylori-uninfected patients: emphasis on differentiated gastric adenocarcinoma. J Gastroenterol. 2022; 57:725–734.
Article9. Kimura K, Takemoto T. An endoscopic recognition of the atrophic border and its significance in chronic gastritis. Endoscopy. 1969; 1:87–97.
Article10. Sakaki N, Momma K, Egawa N, et al. The influence of Helicobacter pylori infection on the progression of gastric mucosal atrophy and occurrence of gastric cancer. Eur J Gastroenterol Hepatol. 1995; 7 Suppl 1:S59–S62.11. Yao K. The endoscopic diagnosis of early gastric cancer. Ann Gastroenterol. 2013; 26:11–22.12. Yao K, Anagnostopoulos GK, Ragunath K. Magnifying endoscopy for diagnosing and delineating early gastric cancer. Endoscopy. 2009; 41:462–467.
Article13. Yoon H, Kim N, Lee HS, et al. Helicobacter pylori-negative gastric cancer in South Korea: incidence and clinicopathologic characteristics. Helicobacter. 2011; 16:382–388.
Article14. Okano A, Kato S, Ohana M. Helicobacter pylori-negative gastric cancer: advanced-stage undifferentiated adenocarcinoma located in the pyloric gland area. Clin J Gastroenterol. 2017; 10:13–17.
Article15. Hayashi J, Yamatsuji T, Suehiro M, et al. Helicobacter pylori-negative advanced gastric cancer arising from the gastric mucosa without inflammation, atrophy, or intestinal metaplasia. Case Rep Gastroenterol. 2022; 16:345–350.
Article16. Takagi A, Ozawa H, Oki M, et al. Helicobacter pylori-negative advanced gastric cancer with massive eosinophilia. Intern Med. 2018; 57:1715–1718.
Article17. Ueyama H, Yao T, Nakashima Y, et al. Gastric adenocarcinoma of fundic gland type (chief cell predominant type): proposal for a new entity of gastric adenocarcinoma. Am J Surg Pathol. 2010; 34:609–619.
Article18. Ueyama H, Yao T, Akazawa Y, et al. Gastric epithelial neoplasm of fundic-gland mucosa lineage: proposal for a new classification in association with gastric adenocarcinoma of fundic-gland type. J Gastroenterol. 2021; 56:814–828.
Article19. Imamura K, Yao K, Nimura S, et al. Characteristic endoscopic findings of gastric adenocarcinoma of fundic-gland mucosa type. Gastric Cancer. 2021; 24:1307–1319.
Article20. Kanesaka T, Uedo N, Yao K, et al. New subtype of gastric adenocarcinoma: mixed fundic and pyloric mucosa-type adenocarcinoma. Clin J Gastroenterol. 2017; 10:224–228.
Article21. Takahashi H, Yao K, Ueo T, et al. Histological subtype of gastric adenocarcinoma: two cases of mixed fundic and pyloric mucosa-type adenocarcinoma. Ecancermedicalscience. 2020; 14:1143.
Article22. Shibagaki K, Fukuyama C, Mikami H, et al. Gastric foveolar-type adenomas endoscopically showing a raspberry-like appearance in the Helicobacter pylori-uninfected stomach. Endosc Int Open. 2019; 7:E784–E791.
Article23. Arai J, Niikura R, Hayakawa Y, et al. Clinicopathological features of gastric cancer with autoimmune gastritis. Biomedicines. 2022; 10:884.
Article24. Nikaido M, Kakiuchi N, Miyamoto S, et al. Indolent feature of Helicobacter pylori-uninfected intramucosal signet ring cell carcinomas with CDH1 mutations. Gastric Cancer. 2021; 24:1102–1114.
Article25. Muraishi J, Miyaoka M, Imamura K, et al. A case of gastric signet-ring cell carcinoma with a long-term retrospective follow-up of 17 years. Clin J Gastroenterol. 2021; 14:1337–1343.
Article26. Takita M, Ohata K, Inamoto R, et al. Endoscopic and histological features of Helicobacter pylori-negative differentiated gastric adenocarcinoma arising in the antrum. JGH Open. 2021; 5:470–477.
Article27. Kushima R, Nimura S. Stomach. In : Fukayama M, Morinaga S, editors. Surgical pathology. 5th ed. Bunkodo;2020. p. 444–515.28. Matsuhisa T, Tsukui T. Relation between reflux of bile acids into the stomach and gastric mucosal atrophy, intestinal metaplasia in biopsy specimens. J Clin Biochem Nutr. 2012; 50:217–221.
Article29. Tatsugami M, Ito M, Tanaka S, et al. Bile acid promotes intestinal metaplasia and gastric carcinogenesis. Cancer Epidemiol Biomarkers Prev. 2012; 21:2101–2107.
Article30. Matsuhisa T, Arakawa T, Watanabe T, et al. Relation between bile acid reflux into the stomach and the risk of atrophic gastritis and intestinal metaplasia: a multicenter study of 2283 cases. Dig Endosc. 2013; 25:519–525.
Article31. Li D, Zhang J, Yao WZ, et al. The relationship between gastric cancer, its precancerous lesions and bile reflux: a retrospective study. J Dig Dis. 2020; 21:222–229.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effectiveness of Helicobacter pylori Eradication before Endoscopic Resection
- Endoscopic Findings of Common Gastritis in Koreans
- Helicobacter pylori-negative Gastric Cancer
- Helicobacter pylori-negative Gastric Mucosa-associated Lymphoid Tissue Lymphoma
- Endoscopic Diagnosis of Early Gastric Cancer and High-Risk Gastritis
