E-learning system to improve the endoscopic diagnosis of early gastric cancer
- Affiliations
-
- 1Department of Endoscopy, Fukuoka University Chikushi Hospital, Fukuoka, Japan
- 2Department of Human Pathology, Juntendo University Graduate School of Medicine, Tokyo, Japan
- 3Department of Gastrointestinal Oncology, Osaka International Cancer Institute, Osaka, Japan
- 4Department of Gastroenterology, Ishikawa Prefectural Central Hospital, Kanazawa, Japan
- 5Department of Molecular-Targeting Cancer Prevention, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, Osaka, Japan
- 6Department of Pathology, Fukuoka University Chikushi Hospital, Fukuoka, Japan
- 7Department of Development, FAST Inc., Tokyo, Japan
- KMID: 2555888
- DOI: http://doi.org/10.5946/ce.2023.087
Abstract
- We developed three e-learning systems for endoscopists to acquire the necessary skills to improve the diagnosis of early gastric cancer (EGC) and demonstrated their usefulness using randomized controlled trials. The subjects of the three e-learning systems were “detection”, “characterization”, and “preoperative assessment”. The contents of each e-learning system included “technique”, “knowledge”, and “obtaining experience”. All e-learning systems proved useful for endoscopists to learn how to diagnose EGC. Lecture videos describing “the technique” and “the knowledge” can be beneficial. In addition, repeating 100 self-study cases allows learners to gain “experience” and improve their diagnostic skills further. Web-based e-learning systems have more advantages than other teaching methods because the number of participants is unlimited. Histopathological diagnosis is the gold standard for the diagnosis of gastric cancer. Therefore, we developed a comprehensive diagnostic algorithm to standardize the histopathological diagnosis of gastric cancer. Once we have successfully shown that this algorithm is helpful for the accurate histopathological diagnosis of cancer, we will complete a series of e-learning systems designed to assess EGC accurately.
Keyword
Figure
-
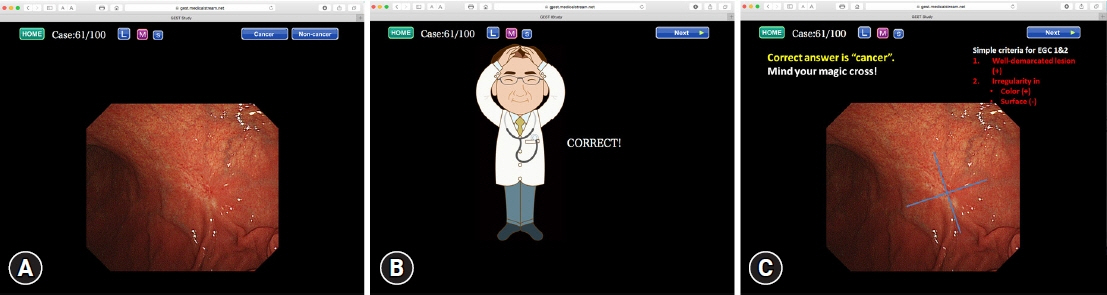
Fig. 1. An example of the self-study cases for the diagnosis of 100 cases. (A) One case comprises a set of three slides. The first slide shows one endoscopic photo where one lesion is present. First, the participant should click to choose whether the lesion is cancerous or noncancerous. (B) Immediately after clicking on their choice, an illustration indicating whether the answer is correct or incorrect appears on the second slide. (C) The third slide indicates brief instructions on characterizing the endoscopic findings to diagnose correctly and shows the original endoscopic image again. Adapted from Yao et al. EBioMedicine 2016;9:140–147, according to the Creative Commons license.5
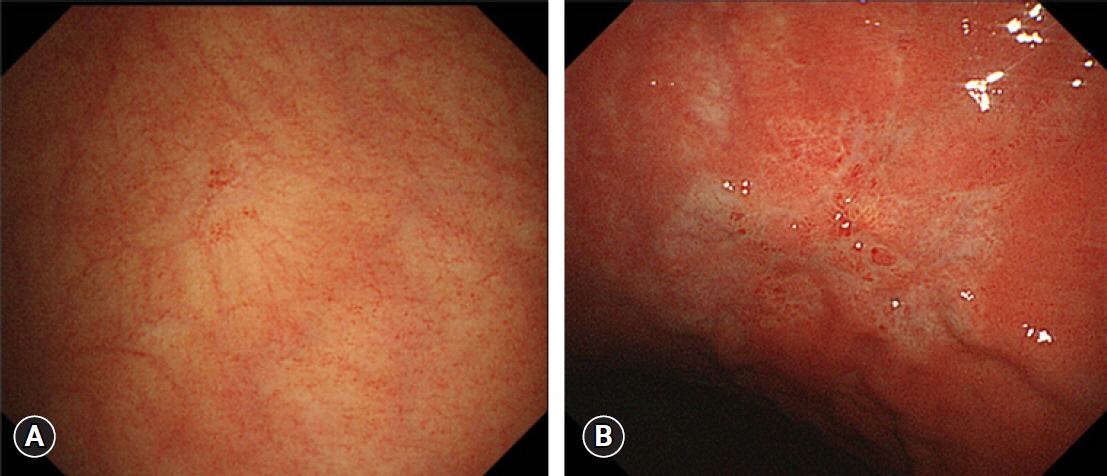
Fig. 2. Example of endoscopic images showing the differences between noncancerous and cancerous lesions according to the color plus surface classification system (CSCS) by conventional white-light imaging. (A) Endoscopic findings of a focal atrophic pale mucosal lesion. According to the CSCS, the lesion is not well demarcated without irregularity in color or surface. Therefore, this lesion is diagnosed as noncancerous. (B) Endoscopic findings of a pale early mucosal lesion. There is a well-demarcated lesion; the distribution of the color is irregular and the surface pattern is irregular. Accordingly, this lesion is diagnosed as cancerous. Adapted from Yao et al. Gastric Cancer 2017;20(Suppl 1):28–38, according to the Creative Commons license.8
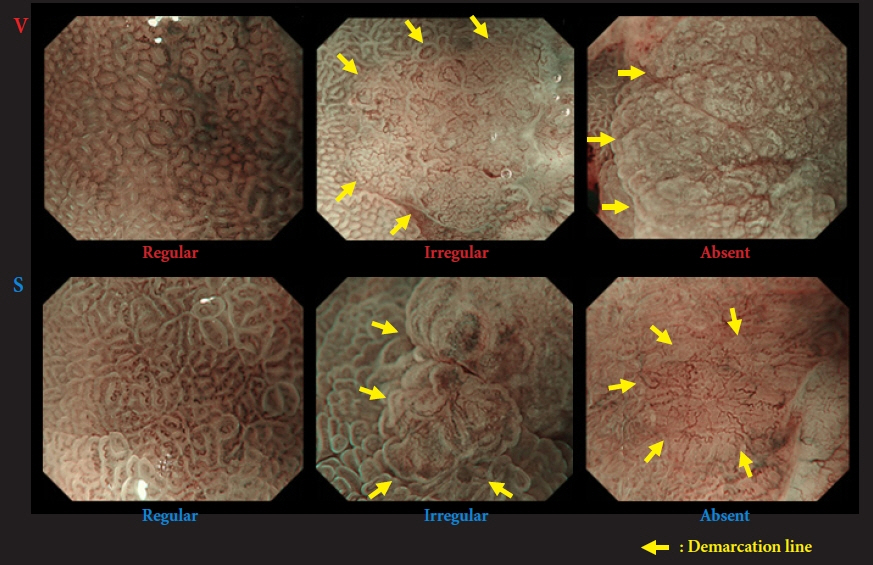
Fig. 3. Vessel plus surface classification system (VSCS) by magnifying narrow-band imaging. Microvascular and microsurface patterns are classified as regular/irregular/absent. If the findings fulfill the following criteria, a cancer diagnosis is made (arrow, demarcation line): (1) presence of an irregular microvascular (MV) pattern with a demarcation line and (2) presence of an irregular microsurface (MS) pattern with a demarcation line. Otherwise, the diagnosis is noncancerous. Adapted from Muto et al. Dig Endosc 2016;28:379–393, according to the Creative Commons license.15
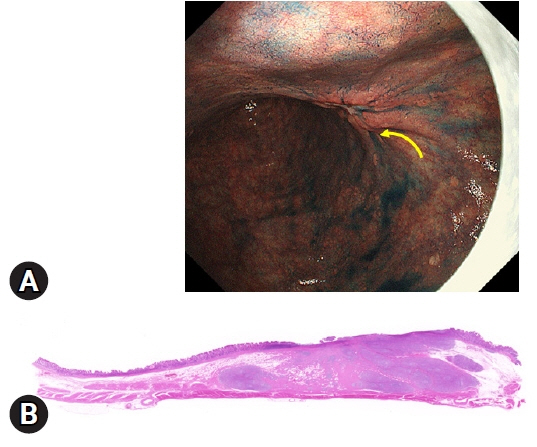
Fig. 4. A representative endoscopic image of early gastric cancer with deep submucosal invasion (T1b2) showing the non-extension sign. (A) The strongly distended gastric wall is gradually elevated toward the submucosa-invasive area (yellow arrow), which has a trapezoid appearance. (B) This endoscopic finding is well supported by the histological findings of the resected specimen. The depth of invasion is 4,500 μm from the muscularis mucosae in this case (hematoxylin and eosin staining, ×20).
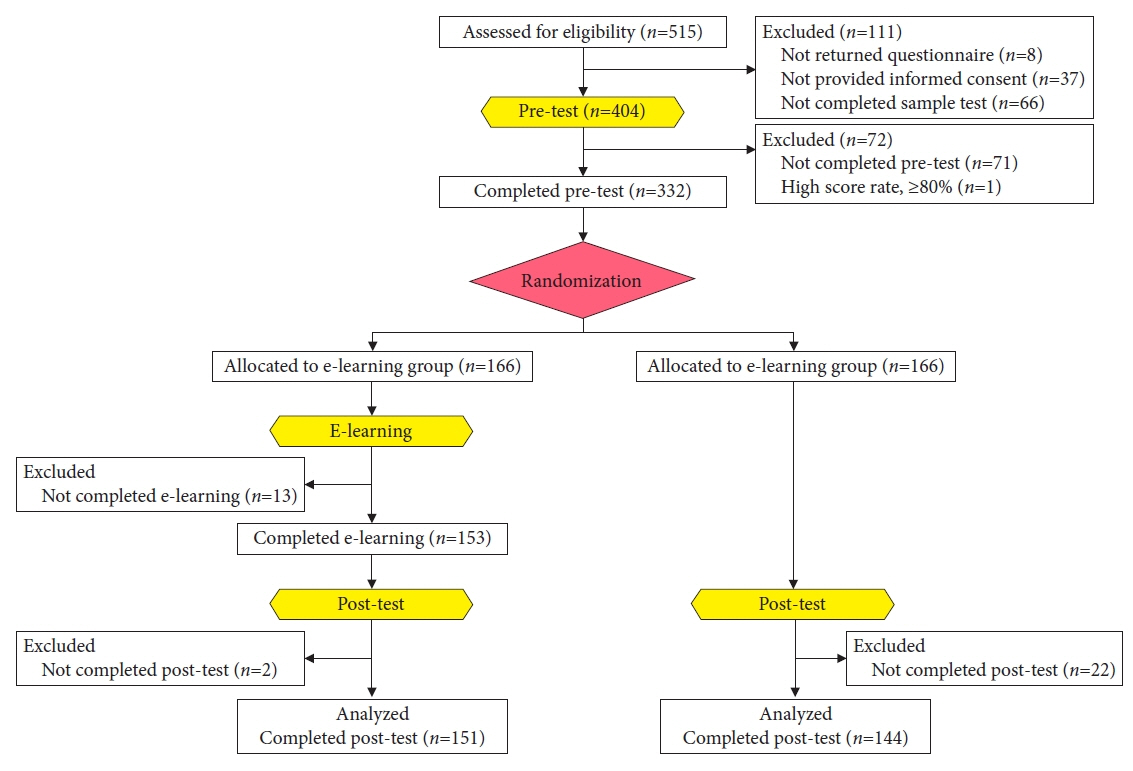
Fig. 5. Flowchart of the enrollment of participants, randomization, and analysis records.
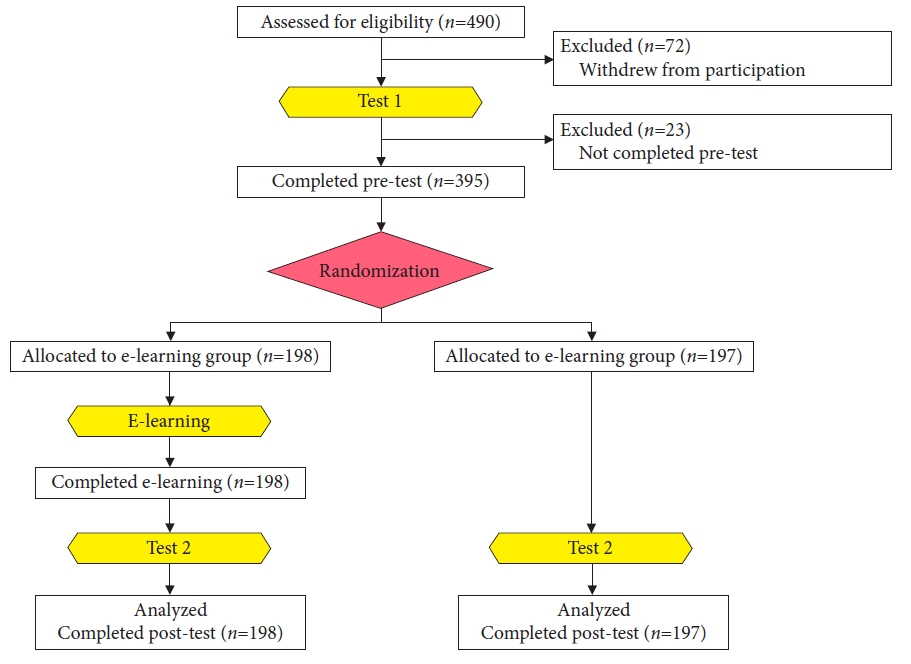
Fig. 6. Flowchart of the enrollment of participants, randomization, and analysis records.
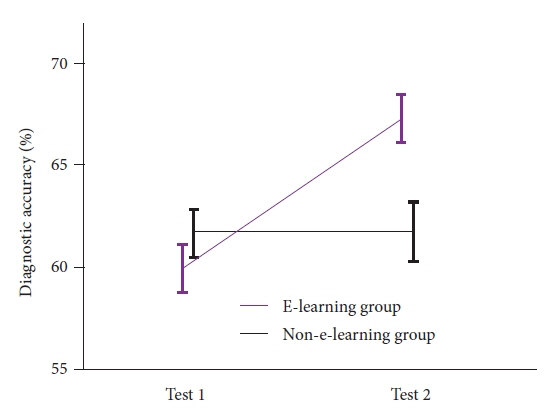
Fig. 7. The changes in accuracy between tests 1 and 2 in the e-learning and non-e-learning groups. The mean accuracy with 95% confidence intervals in tests 1 and 2 for both groups. The change in accuracy in tests 1 and 2 is significantly higher in the e-learning group than in the non-e-learning group (Δ7.4 vs. Δ0.14 points, respectively; p<0.001, unpaired t-test). Adapted from Nakanishi et al. Endoscopy 2017;49:957–967, permission from the publisher.6
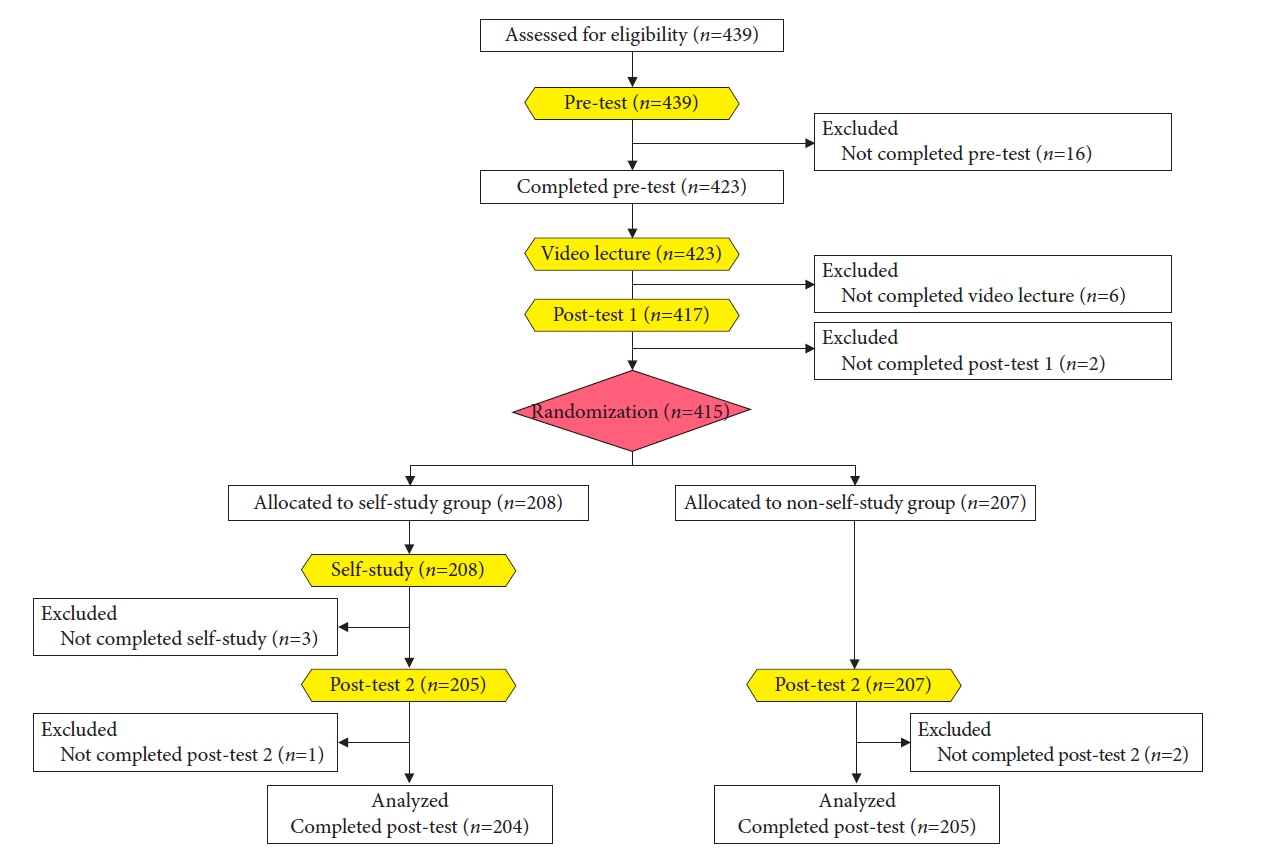
Fig. 8. Flowchart of participants’ enrollment, randomization, and analysis records. The difference with this e-learning study is that to investigate the effect of self-study (accumulating “experience” alone), participants are randomized and allocated to a self-study group or non-self-study group after both groups finish a video lecture showing “technique” and “knowledge”.
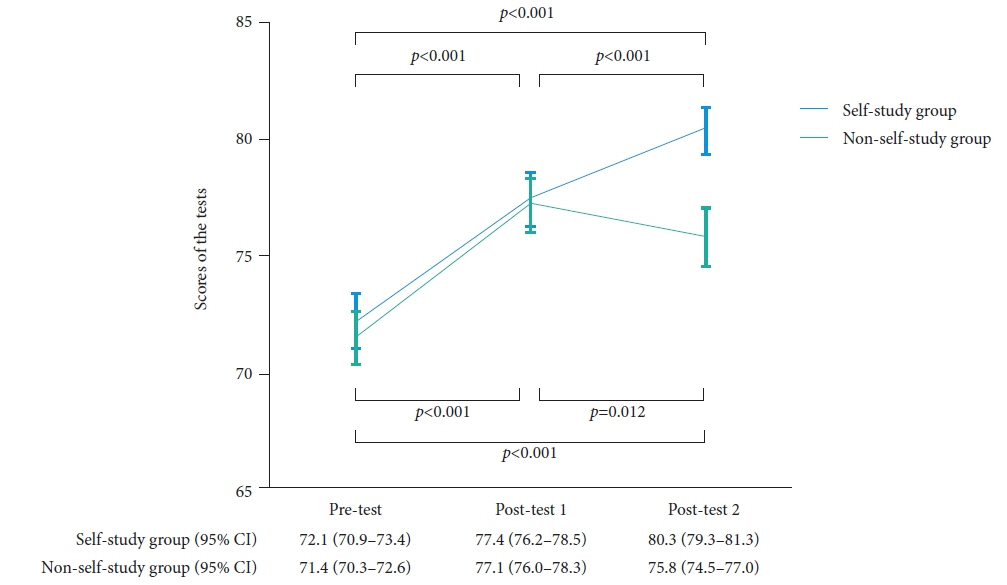
Fig. 9. Changes in the mean scores with 95% confidence intervals (CIs) for the pretest, posttest 1, and posttest 2. The p values are for comparisons between the two tests. In the self-study and non-self-study groups, the mean scores for posttest 2 (80.3 and 75.8) and posttest 1 (77.4 and 77.1) are significantly higher than those for the pretest (72.1 and 71.4; p<0.001, paired t-test). In the self-study group, the mean score for posttest 2 (80.3) is significantly higher than that for posttest 1 (77.4; p<0.001, paired t-test). In the non-self-study group, the mean score for posttest 2 (75.8) is significantly lower than that for posttest 1 (77.1; p=0.012, paired t-test). Adapted from Kato et al. Endosc Int Open 2019;7:E871–E882, according to the Creative Commons license.7
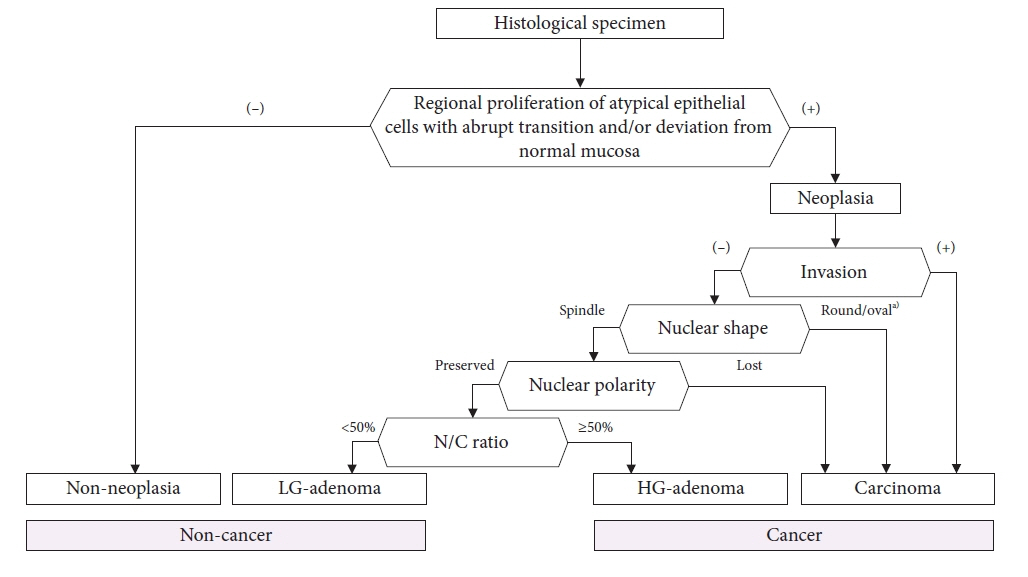
Fig. 10. The algorithm of the histological diagnostic procedure for gastric epithelial lesions. N/C, nucleus to cytoplasmic; LG, low grade; HG, high grade. a)Except for pyloric gland adenoma.
Reference
-
1. Yang L, Ying X, Liu S, et al. Gastric cancer: Epidemiology, risk factors and prevention strategies. Chin J Cancer Res. 2020; 32:695–704.
Article2. Hasuike N, Ono H, Boku N, et al. A non-randomized confirmatory trial of an expanded indication for endoscopic submucosal dissection for intestinal-type gastric cancer (cT1a): the Japan Clinical Oncology Group study (JCOG0607). Gastric Cancer. 2018; 21:114–123.
Article3. Zhang X, Li M, Chen S, et al. Endoscopic screening in Asian countries is associated with reduced gastric cancer mortality: a meta-analysis and systematic review. Gastroenterology. 2018; 155:347–354.
Article4. Yao K. The endoscopic diagnosis of early gastric cancer. Ann Gastroenterol. 2013; 26:11–22.5. Yao K, Uedo N, Muto M, et al. Development of an e-learning system for the endoscopic diagnosis of early gastric cancer: an international multicenter randomized controlled trial. EBioMedicine. 2016; 9:140–147.
Article6. Nakanishi H, Doyama H, Ishikawa H, et al. Evaluation of an e-learning system for diagnosis of gastric lesions using magnifying narrow-band imaging: a multicenter randomized controlled study. Endoscopy. 2017; 49:957–967.7. Kato M, Uedo N, Nagahama T, et al. Self-study of the non-extension sign in an e-learning program improves diagnostic accuracy of invasion depth of early gastric cancer. Endosc Int Open. 2019; 7:E871–E882.8. Yao K, Uedo N, Muto M, et al. Development of an e-learning system for teaching endoscopists how to diagnose early gastric cancer: basic principles for improving early detection. Gastric Cancer. 2017; 20(Suppl 1):28–38.
Article9. Yao K, Doyama H, Tsuji S. Endoscopic characterization of gastric lesions and resection strategy. In : Testoni PA, Inoue H, Wallace MB, editors. Gastrointestinal and pancreatico-biliary diseases: advanced diagnostic and therapeutic endoscopy. Springer;2021. p. 151–170.10. Yoshida N, Doyama H, Yano T, et al. Early gastric cancer detection in high-risk patients: a multicentre randomised controlled trial on the effect of second-generation narrow band imaging. Gut. 2021; 70:67–75.
Article11. Yao K, Anagnostopoulos GK, Ragunath K. Magnifying endoscopy for diagnosing and delineating early gastric cancer. Endoscopy. 2009; 41:462–467.
Article12. Yao K, Uedo N, Kamada T, et al. Guidelines for endoscopic diagnosis of early gastric cancer. Dig Endosc. 2020; 32:663–698.
Article13. Ezoe Y, Muto M, Uedo N, et al. Magnifying narrowband imaging is more accurate than conventional white-light imaging in diagnosis of gastric mucosal cancer. Gastroenterology. 2011; 141:2017–2025.
Article14. Nagahama T, Yao K, Uedo N, et al. Delineation of the extent of early gastric cancer by magnifying narrow-band imaging and chromoendoscopy: a multicenter randomized controlled trial. Endoscopy. 2018; 50:566–576.
Article15. Muto M, Yao K, Kaise M, et al. Magnifying endoscopy simple diagnostic algorithm for early gastric cancer (MESDA-G). Dig Endosc. 2016; 28:379–393.
Article16. Yao K, Doyama H, Gotoda T, et al. Diagnostic performance and limitations of magnifying narrow-band imaging in screening endoscopy of early gastric cancer: a prospective multicenter feasibility study. Gastric Cancer. 2014; 17:669–679.
Article17. Nagahama T, Yao K, Imamura K, et al. Diagnostic performance of conventional endoscopy in the identification of submucosal invasion by early gastric cancer: the "non-extension sign" as a simple diagnostic marker. Gastric Cancer. 2017; 20:304–313.
Article18. Mabe K, Yao K, Nojima M, et al. An educational intervention to improve the endoscopist's ability to correctly diagnose small gastric lesions using magnifying endoscopy with narrow-band imaging. Ann Gastroenterol. 2014; 27:149–155.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Resection of Undifferentiated Early Gastric Cancer
- Endoscopic Treatment of Stomach Cancer
- Endoscopic Resection of Early Gastric Cancer in Korea: Recent Results and Future Directions
- Endoscopic Submucosal Dissection in the Treatment of Patients With Papillary Early Gastric Cancer
- Endoscopic Resection of Early Gastric Cancer
