Central precocious puberty with hypothalamic hamartoma: the first case reports of 2 siblings with different phenotypes of Seckel syndrome 5
- Affiliations
-
- 1Department of Pediatrics, Inha University Hospital, Incheon, Korea
- 2Department of Psychiatry, Inha University Hospital, Incheon, Korea
- 3Department of Orthopedics, Inha University Hospital, Incheon, Korea
- KMID: 2546348
- DOI: http://doi.org/10.6065/apem.2244066.033
Abstract
- Hypothalamic hamartomas (HHs) are nonneoplastic mass lesions located in the hypothalamus that can cause central precocious puberty (CPP) and/or gelastic seizures. Seckel syndrome 5 (OMIM210600, SCKL5) is a rare autosomal recessive genetic spectrum disorder characterized by intrauterine growth retardation, proportionate osteodysplastic primordial dwarfism, a wide range of intellectual disability, "bird-headed" facial features, and microcephaly with various structural brain abnormalities. Two siblings presented with short stature and small head circumference and were diagnosed with SCKL 5. The younger sister had HH with CPP and experienced a slipped capital femoral epiphysis during treatment. The 2 siblings had the same genetic variant but showed different phenotypes, which has not been reported previously; this study also as presents the first cases of SCKL5 diagnosed by genetic confirmation in Korea.
Keyword
Figure
-

Fig. 1. (A) A left-sided growth curve demonstrates the growth velocity of case 1. Her final adult height was 148.9 cm. (B) A right-sided growth curve shows the growth velocity of case 2. When she was 13 years old, her height had reached 144.3 cm.

Fig. 2. (A, B) Magnetic resonance imaging (MRI) findings of case 2. The MRI demonstrates hypothalamic hamartoma (A, arrow) and a pedunculated nonenhancing mass in the tuber cinereum that extended into the suprasellar cistern (B, arrow)
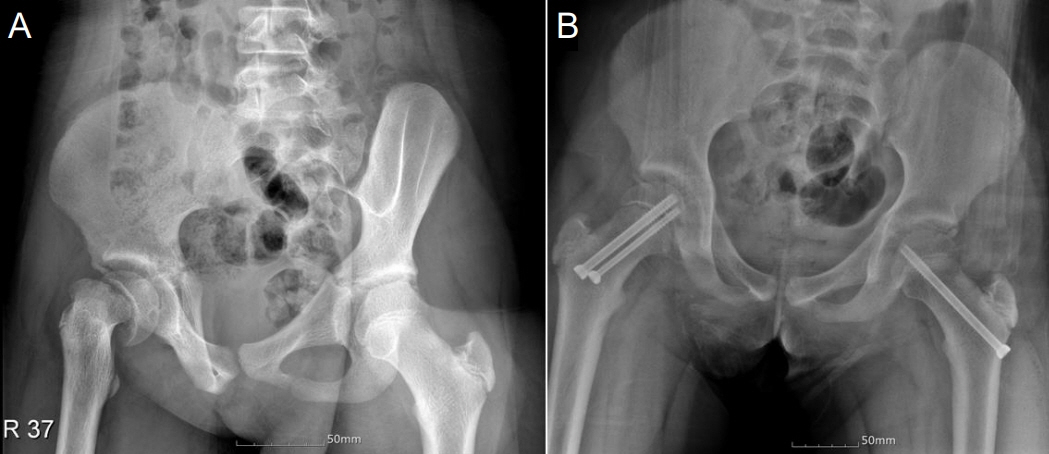
Fig. 3. (A) An x-ray shows right slipped capital femoral epiphysis in case 2. (B) Post fixation of both femur heads.
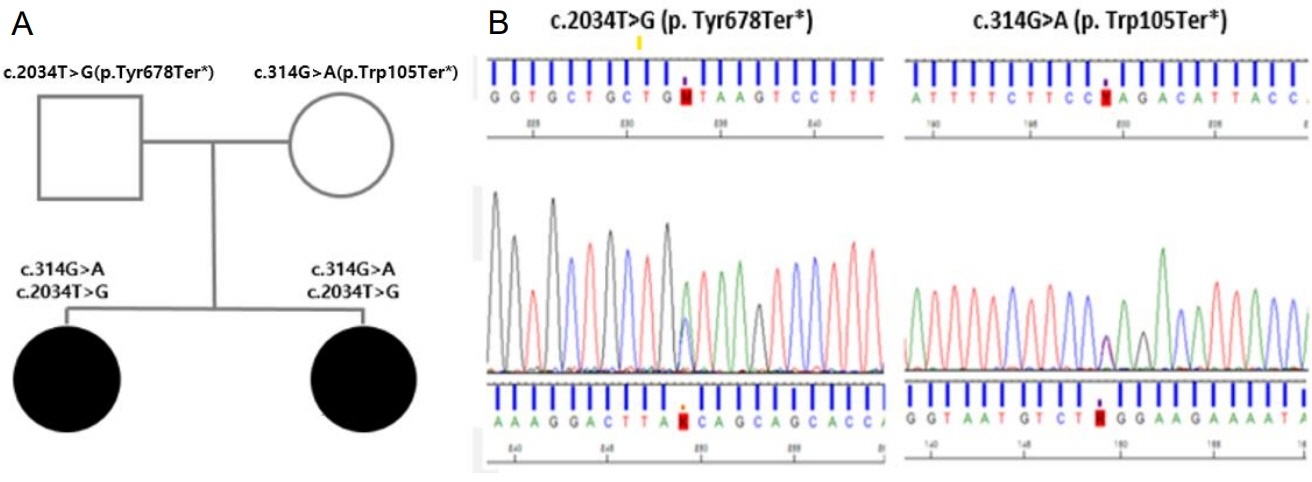
Fig. 4. (A) A pedigree shows that each compound heterozygote variant came from a parent. (B) The pathogenic variants detected in the CEP152 gene (c.2034T>G, p.Tyr678Ter* and c.314G>A, p.Trp105Ter*).
Reference
-
References
1. Arita K, Ikawa F, Kurisu K, Sumida M, Harada K, Uozumi T, et al. The relationship between magnetic resonance imaging findings and clinical manifestations of hypothalamic hamartoma. J Neurosurg. 1999; 91:212–20.2. Kerrigan JF, Parsons A, Tsang C, Simeone K, Coons S, Wu J. Hypothalamic hamartoma: Neuropathology and epileptogenesis. Epilepsia. 2017; 58:22–31.3. Khojah O, Alamoudi S, Aldawsari N, Babgi M, Lary A. Central nervous system vasculopathy and Seckel syndrome: case illustration and systematic review. Childs Nerv Syst. 2021; 37:3847–60.4. Faivre L, Le Merrer M, Lyonnet S, Plauchu H, Dagoneau N, Campos-Xavier AB, et al. Clinical and genetic heterogeneity of Seckel syndrome. Am J Med Genet. 2002; 112:379–83.5. Nigg EA, Raff JW. Centrioles, centrosomes, and cilia in health and disease. Cell. 2009; 139:663–78.6. Capovilla G, Lorenzetti ME, Montagnini A, Borgatti R, Piccinelli P, Giordano L, et al. Seckel's syndrome and malformations of cortical development: report of three new cases and review of the literature. J Child Neurol. 2001; 16:382–6.7. Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015; 17:405–24.8. Savage MO, Storr HL. Balanced assessment of growth disorders using clinical, endocrinological, and genetic approaches. Ann Pediatr Endocrinol Metab. 2021; 26:218–26.9. Green TE, Motelow JE, Bennett MF, Ye Z, Bennett CA, Griffin NG, et al. Sporadic hypothalamic hamartoma is a ciliopathy with somatic and bi-allelic contributions. Hum Mol Genet. 2022; 31:2307–16.10. Jaiswal S, Singh P. Centrosome dysfunction in human diseases. Semin Cell Dev Biol. 2021; 110:113–22.11. Huynh QTV, Ho BT, Le NQK, Trinh TH, Lam LHT, Nguyen NTK, et al. Pathological brain lesions in girls with central precocious puberty at initial diagnosis in Southern Vietnam. Ann Pediatr Endocrinol Metab. 2022; 27:105–12.12. Birkebaek NH, Wolthers OD, Heuch C, Balslev T, Flyvbjerg A, Frystyk J. Growth hormone treatment, final height, insulin-like growth factors, ghrelin, and adiponectin in four siblings with Seckel syndrome. J Pediatr Endocrinol Metab. 2011; 24:995–1000.13. Inman M, Hursh BE, Mokashi A, Pinto T, Metzger DL, Cummings EA. Occurrence of slipped capital femoral epiphysis in children undergoing gonadotropin-releasing hormone agonist therapy for the treatment of central precocious puberty. Horm Res Paediatr. 2013; 80:64–8.14. Wang SY, Tung YC, Tsai WY, Chien YH, Lee JS, Hwu WL. Slipped capital femoral epiphysis as a complication of growth hormone therapy. J Formos Med Assoc. 2007; 106(2 Suppl):S46–50.15. Lee JW, Kim HJ, Choe YM, Kang HS, Kim SK, Jun YH, et al. Significant adverse reactions to long-acting gonadotropinreleasing hormone agonists for the treatment of central precocious puberty and early onset puberty. Ann Pediatr Endocrinol Metab. 2014; 19:135–40.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hypothalamic hamartoma associated with precocious puberty: case report
- A Case Report of Precocious Puberty in Children Associated with Hypothalamic Hamartoma in Neurofibromatosis Type 1
- Hypothalamic Tumors Causing Precocious Puberty
- An 11-month-old girl with central precocious puberty caused by hypothalamic hamartoma
- Treatment of Hypothalamic Hamartoma
