A Case of IgG4-Related Disease With Sinonasal Involvement Presenting With Decreased Visual Acuity
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Bucheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea
- KMID: 2540859
- DOI: http://doi.org/10.18787/jr.2023.00008
Abstract
- IgG4-related disease (IgG4-RD) is a systemic inflammatory disease characterized by IgG4-positive plasma cell and T lymphocyte infiltration of multiple organs. It commonly involves the pancreas, lacrimal glands, and salivary glands, and it has been rarely reported in the sinonasal cavity. We herein report the case of a 47-year-old male patient whose chief complaint was decreased visual acuity. A tumefactive mass was found on imaging studies, originating from the sinonasal cavity and invading the orbit, kidney, and meninges. The mass was resected through endoscopic sinus surgery and was pathologically confirmed to be IgG4-RD. The patient was treated with steroid therapy and showed clinical improvement.
Figure
-
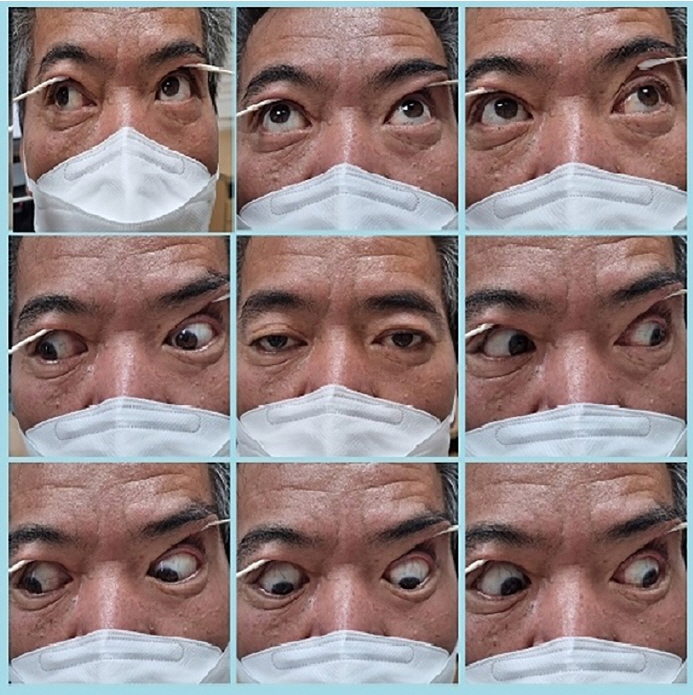
Fig. 1. Extraocular movement. The patient shows normal extraocular muscle function.
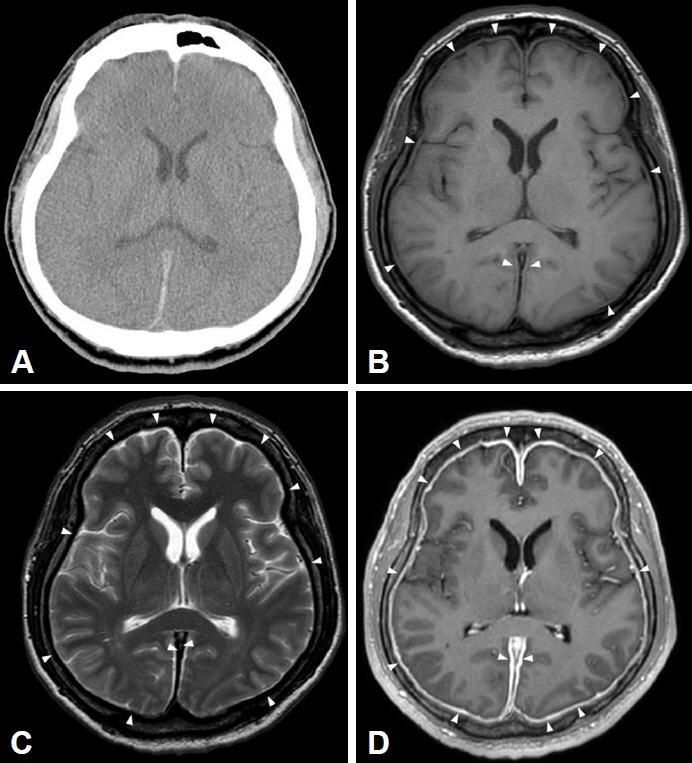
Fig. 2. Initial brain computed tomography (CT) and magnetic resonance imaging (MRI). A: Non-contrast brain CT shows no definite abnormality. B: T1-weighted MRI shows isointense dural thickening (white arrowheads). C: T2-weighted MRI shows markedly hypointense dural thickening (white arrowheads). D: Contrast-enhanced T1-weighted MRI shows smooth, homogeneous pachymeningeal enhancement along both cerebral hemispheres (white arrowheads).
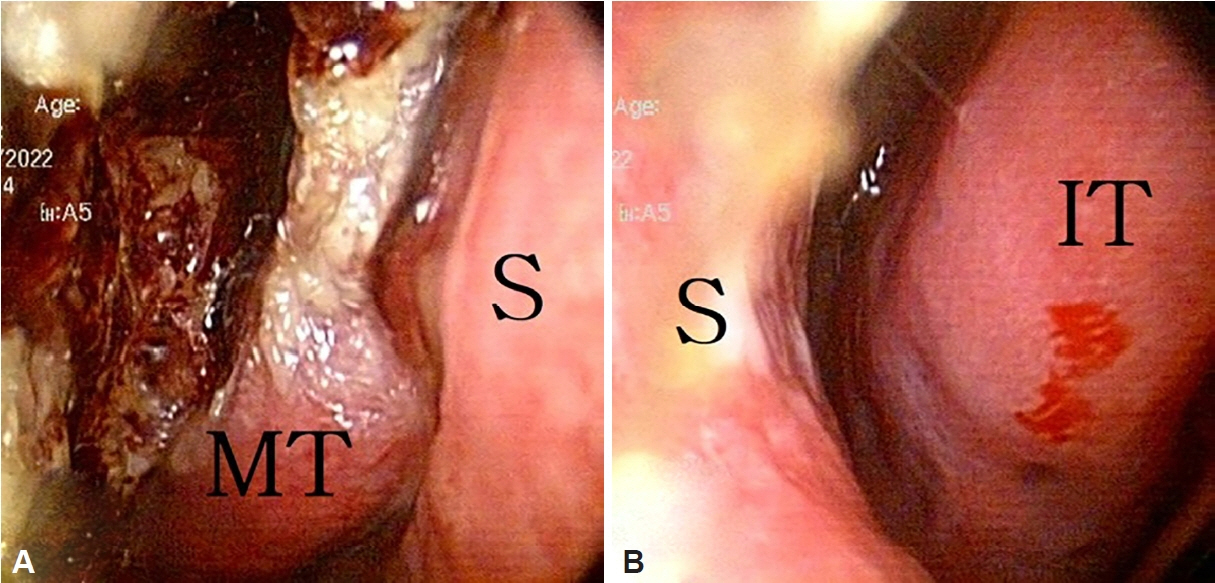
Fig. 3. Preoperative endoscopic findings of the nasal cavity. A: The right nasal cavity is filled with crust and purulent discharge. B: The left nasal cavity shows inferior turbinate hypertrophy. S, septum; MT, middle turbinate; IT, inferior turbinate.
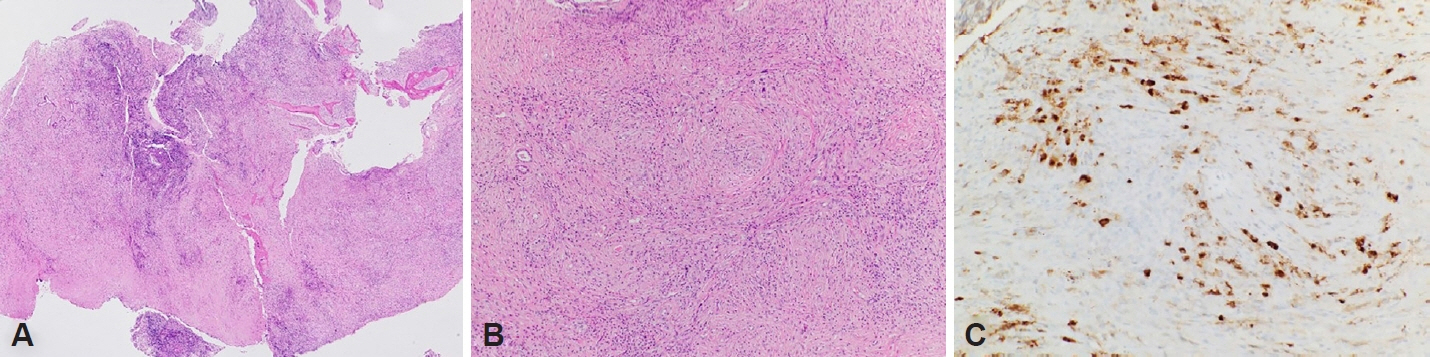
Fig. 4. Pathologic findings of the sinonasal cavity. A: Low-power view of dense lymphoplasmacytic infiltrate and hyaline fibrosis (hematoxylin and eosin staining, ×40 magnification). B: High-power view of storiform fibrosis and lymphoplasmacytic infiltrate (hematoxylin and eosin staining, ×100 magnification). C: High-power IgG4 immunohistochemical stain shows an increased IgG4 cell count and increased IgG4/IgG ratio (immunohistochemical staining for IgG4, ×200 magnification).

Fig. 5. Contrast-enhanced abdominal computed tomography shows hypodense, hypovascular lesions in the right kidney, suggestive of IgG4-related kidney disease.
Reference
-
References
1. Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, et al. A novel clinical entity, IgG4-related disease (IgG4RD): general concept and details. Mod Rheumatol. 2012; 22(1):1–14.
Article2. Hamano H, Kawa S, Horiuchi A, Unno H, Furuya N, Akamatsu T, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001; 344(10):732–8.
Article3. Mulholland GB, Jeffery CC, Satija P, Côté DW. Immunoglobulin G4-related diseases in the head and neck: a systematic review. J Otolaryngol Head Neck Surg. 2015; 44(1):24.
Article4. Cheuk W, Chan JK. IgG4-related sclerosing disease: a critical appraisal of an evolving clinicopathologic entity. Adv Anat Pathol. 2010; 17(5):303–32.5. Umehara H, Okazaki K, Kawa S, Takahashi H, Goto H, Matsui S, et al. The 2020 revised comprehensive diagnostic (RCD) criteria for IgG4-RD. Mod Rheumatol. 2021; 31(3):529–33.
Article6. Park DH, Kim MH, Oh HB, Kwon OJ, Choi YJ, Lee SS, et al. Substitution of aspartic acid at position 57 of the DQbeta1 affects relapse of autoimmune pancreatitis. Gastroenterology. 2008; 134(2):440–6.
Article7. Guarneri F, Guarneri C, Benvenga S. Helicobacter pylori and autoimmune pancreatitis: role of carbonic anhydrase via molecular mimicry? J Cell Mol Med. 2005; 9(3):741–4.
Article8. Frulloni L, Lunardi C, Simone R, Dolcino M, Scattolini C, Falconi M, et al. Identification of a novel antibody associated with autoimmune pancreatitis. N Engl J Med. 2009; 361(22):2135–42.
Article9. Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med. 2012; 366(6):539–51.
Article10. Kawano M, Saeki T, Nakashima H, Nishi S, Yamaguchi Y, Hisano S, et al. Proposal for diagnostic criteria for IgG4-related kidney disease. Clin Exp Nephrol. 2011; 15(5):615–26.
Article11. Lindstrom KM, Cousar JB, Lopes MB. IgG4-related meningeal disease: clinico-pathological features and proposal for diagnostic criteria. Acta Neuropathol. 2010; 120(6):765–76.
Article12. Kamisawa T, Okazaki K, Kawa S, Ito T, Inui K, Irie H, et al. Amendment of the Japanese consensus guidelines for autoimmune pancreatitis, 2013 III. Treatment and prognosis of autoimmune pancreatitis. J Gastroenterol. 2014; 49(6):961–70.
Article13. Ueno M, Nakano K, Miyagawa I, Tanaka Y. Five cases of IgG4-related disease with nasal mucosa and sinus involvement. Intern Med. 2020; 59(15):1905–11.
Article14. Yunyun F, Yu P, Panpan Z, Xia Z, Linyi P, Jiaxin Z, et al. Efficacy and safety of low dose mycophenolate mofetil treatment for immunoglobulin G4-related disease: a randomized clinical trial. Rheumatology (Oxford). 2019; 58(1):52–60.
Article15. Carruthers MN, Stone JH, Deshpande V, Khosroshahi A. Development of an IgG4-RD responder index. Int J Rheumatol. 2012; 2012:259408.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Immunoglobulin G4 Related Ophthalmic Disease Presenting as Diplopia and Headache
- A Case of IgG4-Related Sclerosing Disease Involving the Optic Nerve
- A Case of IgG4-Related Lung Disease Presenting as Interstitial Lung Disease
- A Case of IgG4-Related Pseudotumor in Larynx
- A Case of IgG4-Related Pancreas and Kidney Disease Mimicking a Renal Pelvic Malignancy
