Impact of intradialytic hypotension on mortality following the transition from continuous renal replacement therapy to intermittent hemodialysis
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea
- KMID: 2540318
- DOI: http://doi.org/10.4266/acc.2022.00948
Abstract
- Background
The transition of dialysis modalities from continuous renal replacement therapy (CRRT) to intermittent hemodialysis (iHD) is frequently conducted during the recovery phase of critically ill patients with acute kidney injury. Herein, we addressed the occurrence of intradialytic hypotension (IDH) after this transition, and its association with the mortality risk.
Methods
A total of 541 patients with acute kidney injury who attempted to transition from CRRT to iHD at Seoul National University Hospital, Korea from 2010 to 2020 were retrospectively collected. IDH was defined as a discontinuation of dialysis because of hemodynamic instability plus a nadir systolic blood pressure <90 mm Hg or a decrease in systolic blood pressure ≥30 mm Hg during the first session of iHD. Odds ratios (ORs) of outcomes, such as in-hospital mortality and weaning from RRT, were measured using a logistic regression model after adjusting for multiple variables.
Results
IDH occurred in 197 patients (36%), and their mortality rate (44%) was higher than that of those without IDH (19%; OR, 2.64; 95% confidence interval [CI], 1.70–4.08). For patients exhibiting IDH, the iHD sessions delayed successful weaning from RRT (OR, 0.62; 95% CI, 0.43–0.90) compared with sessions on those without IDH. Factors such as low blood pressure, high pulse rate, low urine output, use of mechanical ventilations and vasopressors, and hypoalbuminemia were associated with IDH risk.
Conclusions
IDH occurrence following the transition from CRRT to iHD is associated with high mortality and delayed weaning from RRT.
Keyword
Figure
-
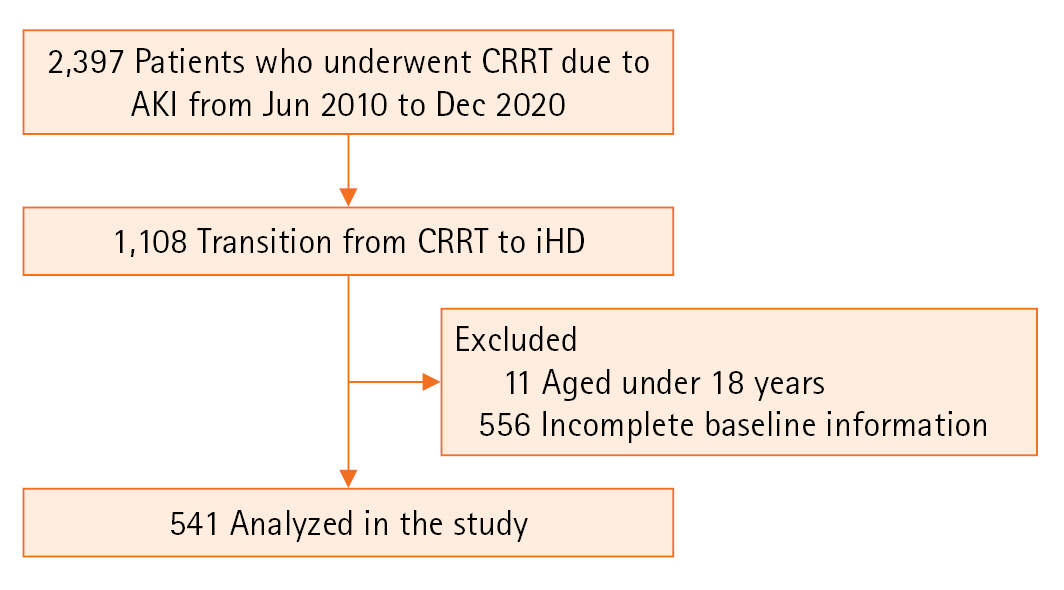
Figure 1. Flowchart of selection criteria. CRRT: continuous renal replacement therapy; AKI: acute kidney injury; iHD: intermittent hemodialysis.

Figure 2. Kaplan-Meier survival curves between patients with and without intradialytic hypotension (IDH). IDH was defined as a discontinuation of dialysis because of hemodynamic instability plus a nadir systolic blood pressure <90 mm Hg (IDH-A) or a decrease in systolic blood pressure ≥30 mm Hg (IDH-B).

Figure 3. Kaplan-Meier curves of the weaning rate from renal replacement therapy (RRT). IDH: intradialytic hypotension.

Figure 4. Forest plot of subgroup analyses for the odds ratio (OR) of the renal replacement therapy weaning rate in the group with intradialytic hypotension compared with that of the group without intradialytic hypotension. CI: confidence interval; AKI: acute kidney injury; SOFA: Sequential Organ Failure Assessment.
Reference
-
1. Cerdá J, Lameire N, Eggers P, Pannu N, Uchino S, Wang H, et al. Epidemiology of acute kidney injury. Clin J Am Soc Nephrol. 2008; 3:881–6.
Article2. Hsu RK, McCulloch CE, Dudley RA, Lo LJ, Hsu CY. Temporal changes in incidence of dialysis-requiring AKI. J Am Soc Nephrol. 2013; 24:37–42.
Article3. Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, et al. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005; 294:813–8.
Article4. Tolwani A. Continuous renal-replacement therapy for acute kidney injury. N Engl J Med. 2012; 367:2505–14.
Article5. Lo LJ, Go AS, Chertow GM, McCulloch CE, Fan D, Ordoñez JD, et al. Dialysis-requiring acute renal failure increases the risk of progressive chronic kidney disease. Kidney Int. 2009; 76:893–9.
Article6. Duran PA, Concepcion LA. Survival after acute kidney injury requiring dialysis: long-term follow up. Hemodial Int. 2014; 18 Suppl 1:S1–6.
Article7. Chawla LS, Amdur RL, Shaw AD, Faselis C, Palant CE, Kimmel PL. Association between AKI and long-term renal and cardiovascular outcomes in United States veterans. Clin J Am Soc Nephrol. 2014; 9:448–56.
Article8. Wu VC, Wu CH, Huang TM, Wang CY, Lai CF, Shiao CC, et al. Long-term risk of coronary events after AKI. J Am Soc Nephrol. 2014; 25:595–605.
Article9. Bellomo R, Kellum JA, La Manna G, Ronco C. 40 Years of continuous renal replacement therapy. Karger;2018.10. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012; 120:c179–84.
Article11. Schefold JC, von Haehling S, Pschowski R, Bender T, Berkmann C, Briegel S, et al. The effect of continuous versus intermittent renal replacement therapy on the outcome of critically ill patients with acute renal failure (CONVINT): a prospective randomized controlled trial. Crit Care. 2014; 18:R11.
Article12. Chawla LS, Bellomo R, Bihorac A, Goldstein SL, Siew ED, Bagshaw SM, et al. Acute kidney disease and renal recovery: consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup. Nat Rev Nephrol. 2017; 13:241–57.
Article13. Nash DM, Przech S, Wald R, O’Reilly D. Systematic review and meta-analysis of renal replacement therapy modalities for acute kidney injury in the intensive care unit. J Crit Care. 2017; 41:138–44.
Article14. Karkar A, Ronco C. Prescription of CRRT: a pathway to optimize therapy. Ann Intensive Care. 2020; 10:32.
Article15. Brownback CA, Fletcher P, Pierce LN, Klaus S. Early mobility activities during continuous renal replacement therapy. Am J Crit Care. 2014; 23:348–51.
Article16. Srisawat N, Lawsin L, Uchino S, Bellomo R, Kellum JA, BEST Kidney Investigators. Cost of acute renal replacement therapy in the intensive care unit: results from The Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) study. Crit Care. 2010; 14:R46.
Article17. Sars B, van der Sande FM, Kooman JP. Intradialytic hypotension: mechanisms and outcome. Blood Purif. 2020; 49:158–67.
Article18. VA/NIH Acute Renal Failure Trial Network, Palevsky PM, Zhang JH, O’Connor TZ, Chertow GM, Crowley ST, et al. Intensity of renal support in critically ill patients with acute kidney injury. N Engl J Med. 2008; 359:7–20.
Article19. Silversides JA, Pinto R, Kuint R, Wald R, Hladunewich MA, Lapinsky SE, et al. Fluid balance, intradialytic hypotension, and outcomes in critically ill patients undergoing renal replacement therapy: a cohort study. Crit Care. 2014; 18:624.
Article20. Tonelli M, Astephen P, Andreou P, Beed S, Lundrigan P, Jindal K. Blood volume monitoring in intermittent hemodialysis for acute renal failure. Kidney Int. 2002; 62:1075–80.21. Shawwa K, Kompotiatis P, Jentzer JC, Wiley BM, Williams AW, Dillon JJ, et al. Hypotension within one-hour from starting CRRT is associated with in-hospital mortality. J Crit Care. 2019; 54:7–13.22. Jones AE, Trzeciak S, Kline JA. The Sequential Organ Failure Assessment score for predicting outcome in patients with severe sepsis and evidence of hypoperfusion at the time of emergency department presentation. Crit Care Med. 2009; 37:1649–54.23. Sundararajan V, Henderson T, Perry C, Muggivan A, Quan H, Ghali WA. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J Clin Epidemiol. 2004; 57:1288–94.24. Flythe JE, Xue H, Lynch KE, Curhan GC, Brunelli SM. Association of mortality risk with various definitions of intradialytic hypotension. J Am Soc Nephrol. 2015; 26:724–34.25. Beaubien-Souligny W, Yang Y, Burns KE, Friedrich JO, Meraz-Muñoz A, Clark EG, et al. Intra-dialytic hypotension following the transition from continuous to intermittent renal replacement therapy. Ann Intensive Care. 2021; 11:96.26. Douvris A, Zeid K, Hiremath S, Bagshaw SM, Wald R, Beaubien-Souligny W, et al. Mechanisms for hemodynamic instability related to renal replacement therapy: a narrative review. Intensive Care Med. 2019; 45:1333–46.27. Kaysen GA, Dubin JA, Müller HG, Rosales L, Levin NW, Mitch WE, et al. Inflammation and reduced albumin synthesis associated with stable decline in serum albumin in hemodialysis patients. Kidney Int. 2004; 65:1408–15.28. Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. N Engl J Med. 1999; 340:448–54.29. Macedo E, Karl B, Lee E, Mehta RL. A randomized trial of albumin infusion to prevent intradialytic hypotension in hospitalized hypoalbuminemic patients. Crit Care. 2021; 25:18.30. Manns M, Sigler MH, Teehan BP. Intradialytic renal haemodynamics: potential consequences for the management of the patient with acute renal failure. Nephrol Dial Transplant. 1997; 12:870–2.31. Kelleher SP, Robinette JB, Miller F, Conger JD. Effect of hemorrhagic reduction in blood pressure on recovery from acute renal failure. Kidney Int. 1987; 31:725–30.32. Augustine JJ, Sandy D, Seifert TH, Paganini EP. A randomized controlled trial comparing intermittent with continuous dialysis in patients with ARF. Am J Kidney Dis. 2004; 44:1000–7.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Renal Replacement Therapies on the Outcomes of Acute Renal Failure Patients in ICU
- Use of fludrocortisone for intradialytic hypotension
- Impacts of Coronary Artery Calcification on Intradialytic Blood Pressure Patterns in Patients Receiving Maintenance Hemodialysis
- System of integrating biosignals during hemodialysis: the CONTINUAL (Continuous mOnitoriNg viTal sIgN dUring hemodiALysis) registry
- Impact of Dialysis Modalities on Survival of Acute Renal Failure in Intensive Care Unit
