Fracture of a Flow Diverter in the Cervical Internal Carotid Artery Due to Eagle Syndrome
- Affiliations
-
- 1Department of Neuroradiology, Christian Doppler Medical Center, Paracelsus Medical University, Salzburg, Austria
- 2Department of Neurology, Christian Doppler Medical Center, Paracelsus Medical University, Centre for Cognitive Neuroscience Salzburg, Salzburg, Austria
- 3Institute of Neurointervention, Paracelsus Medical University, Salzburg, Austria
- KMID: 2539950
- DOI: http://doi.org/10.5469/neuroint.2022.00409
Abstract
- In Eagle syndrome, elongated styloid processes may provoke internal carotid dissection and pseudoaneurysm causing stroke and data regarding possible complications or long-term results of pseudoaneurysm treatment using a flow diverter are limited. We report a case of a dissection-related pseudoaneurysm in the left cervical carotid artery treated by implantation of a flow diverter. Follow-up imaging of the flow diverter showed fracture of a continuous radiopaque marker at 3 months and fracture of a second continuous radiopaque marker at 7 months, while contrasting of the vessel was preserved. At the time of angiographic control (8 months after implantation), the flow diverter and the extracranial left internal carotid artery were occluded, and the patient did not experience any symptoms throughout the period.
Keyword
Figure
-
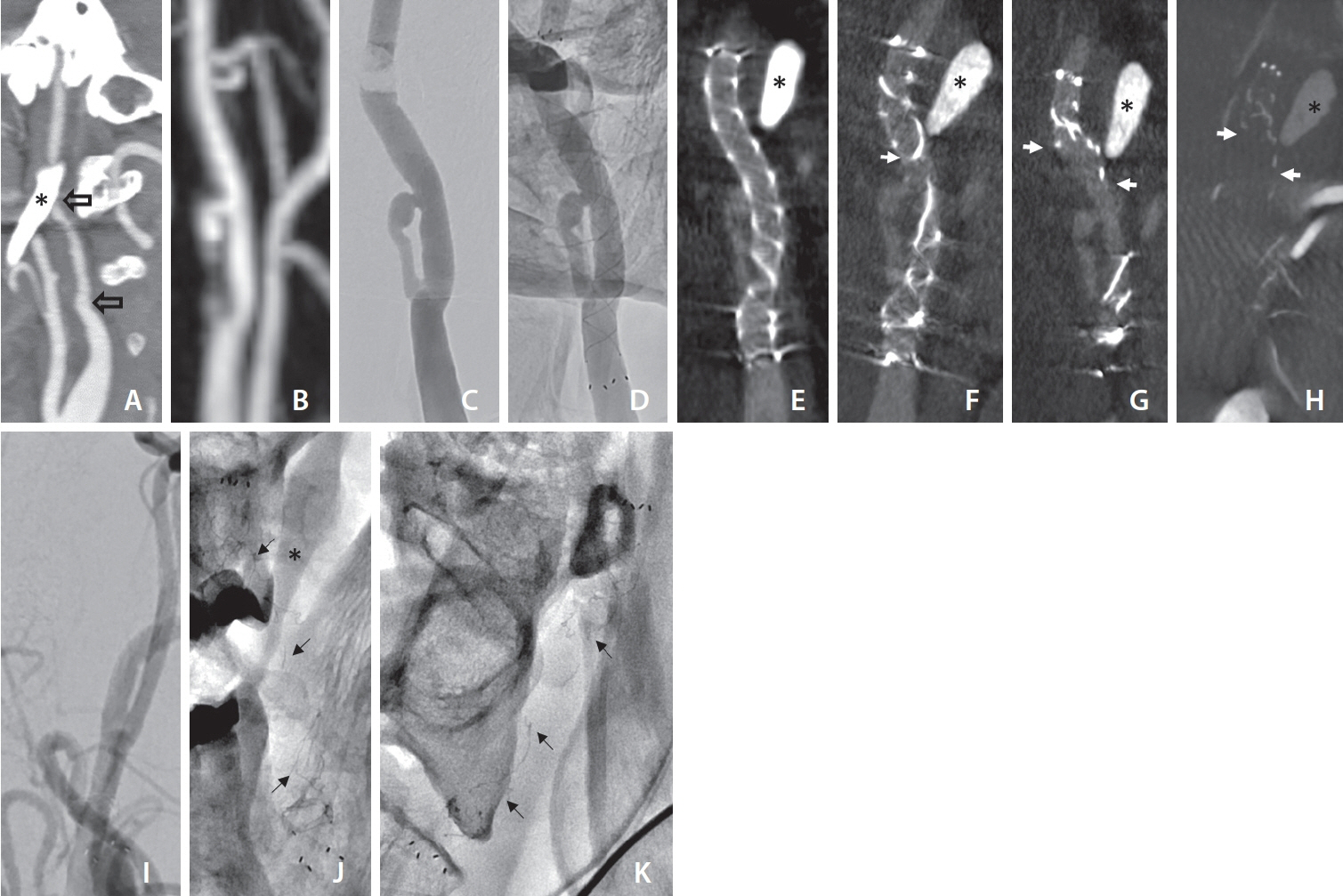
Fig. 1. Sagittal images of computed tomography (CT) angiography at first presentation of a patient with minor stroke showing the elongated styloid process (asterisk) and a caliber reduction of the left internal carotid artery (ICA) secondary to dissection. (A) The blank arrows indicate the proximal and distal entry of the dissection, later to become the pseudoaneurysm. (B) Contrast-enhanced magnetic resonance angiography (posteroanterior [PA] view) of the left ICA showing a pseudoaneurysm after 6 months. Digital subtraction angiography (DSA) image of the left carotid artery pseudoaneurysm before (C) and corresponding non-subtracted angiography image after (D) implantation of the flow diverter. Coronal multiplanar reconstruction of flat-panel CT with intravenous contrast: on day 1 (E), at 3 months (F), and at 7 months (G) after flow diverter implantation. Note: despite the implanted flow diverter, the pseudoaneurysm still fills with contrast agent (E–G). (H) Coronal multiplanar reconstruction of flat-panel CT after intra-arterial contrast medium injection in the left ICA at 8 months after implantation. The white arrows on the follow-up images indicate the fractured and retracted distal radiopaque struts of the flow diverter. (I) DSA image (PA view) of the flow diverter 8 months after implantation showing occlusion of the device and the ICA. Single shot X-ray of the fractured flow diverter in PA (J) and lateral view (K). The black arrows point to fragments of the radiopaque struts of the flow diverter.
Reference
-
1. Balbuena L Jr, Hayes D, Ramirez SG, Johnson R. Eagle‘s syndrome (elongated styloid process). South Med J. 1997; 90:331–334.
Article2. Zamboni P, Scerrati A, Menegatti E, Galeotti R, Lapparelli M, Traina L, et al. The Eagle jugular syndrome. BMC Neurol. 2019; 19:333.
Article3. Baptista-Sincos APW, Simplício AB, Sincos IR, Leaderman A, Neto FS, Moraes A, et al. Flow-diverting stent in the treatment of cervical carotid dissection and pseudoaneurysm: review of literature and case report. Ann Vasc Surg. 2018; 46:372–379.
Article4. Beaty N, Patel M, Martinez C, Hollis L. Use of flow diverter stent for treatment of a cervical carotid artery dissection and pseudoaneurysm causing Horner‘s syndrome. BMJ Case Rep. 2021; 14:e241156.
Article5. Rizwan M, Smith C, Faro S, Malas MB. Transcarotid artery stenting for carotid artery pseudoaneurysm using flow reversal technique. J Vasc Surg Cases Innov Tech. 2018; 4:115–118.
Article6. Diana F, Frauenfelder G, Saponiero R, Iaconetta G, Romano DG. Endovascular flow diversion in cervical internal carotid artery dissections. World Neurosurg. 2022; 162:10.
Article7. Dao A, Karnezis S, Lane JS 3rd, Fujitani RM, Saremi F. Eagle syndrome presenting with external carotid artery pseudoaneurysm. Emerg Radiol. 2011; 18:263–265.
Article8. Rocco R, Bower TC, Macedo TA, Kasperbauer J, Morris J, Mendes BC. Asymptomatic right internal carotid artery pseudoaneurysm and Eagle‘s syndrome. J Vasc Surg. 2022; 75:695–696.
Article9. Sultan S, Acharya Y, Soliman O, Hynes N. Stylohyoid Eagle syndrome and EXTracranial INternal Carotid arTery pseudoaneurysms (EXTINCT) with internal jugular vein nutcracker syndrome: a challenging clinical scenario. BMJ Case Rep. 2022; 15:e249558.
Article10. Hooker JD, Joyner DA, Farley EP, Khan M. Carotid stent fracture from stylocarotid syndrome. J Radiol Case Rep. 2016; 10:1–8.11. Tan D, Crockett MT, Chiu AHY. Delayed tine displacement of a CASPER carotid artery stent due to styloid process compression. Clin Neuroradiol. 2019; 29:567–569.
Article12. Duarte-Celada WR, Jin D, Neves G, Windisch T. Bilateral carotid dissection due to Eagle syndrome in a young female. eNeurologicalSci. 2021; 24:100353.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Symptomatic Post Endarterectomy Common Carotid Artery Pseudoaneurysm Treated with Combination of Flow Diverter Implantation and Carotid Stenting
- Kinking of Flow Diverter in a Giant Wide-Necked Supraclinoid Internal Carotid Artery Aneurysm
- Internal Carotid Artery Reconstruction with a “Mega Flow Diverterâ€: First Experience with the 6×50 mm DERIVO Embolization Device
- Delayed fatal rupture of vertebral artery after treated with flow-diverter in fibromuscular dysplasia patient: A case report and review of the literature
- Salvage flow diverter stent across the posterior communicating artery for persistent retrograde filling of a giant internal carotid artery aneurysm after parent vessel occlusion
