Assessment and Comparison of Three Dimensional Exoscopes for Near-Infrared Fluorescence-Guided Surgery Using Second-Window Indocyanine-Green
- Affiliations
-
- 1Department of Neurosurgery, Hospital of the University of Pennsylvania, Philadelphia, PA, USA
- 2Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, USA
- KMID: 2531626
- DOI: http://doi.org/10.3340/jkns.2021.0202
Abstract
Objective
: Compared to microscopes, exoscopes have advantages in field-depth, ergonomics, and educational value. Exoscopes are especially well-poised for adaptation into fluorescence-guided surgery (FGS) due to their excitation source, light path, and image processing capabilities. We evaluated the feasibility of near-infrared FGS using a 3-dimensional (3D), 4 K exoscope with nearinfrared fluorescence imaging capability. We then compared it to the most sensitive, commercially-available near-infrared exoscope system (3D and 960 p). In-vitro and intraoperative comparisons were performed.
Methods
: Serial dilutions of indocyanine-green (1–2000 μg/mL) were imaged with the 3D, 4 K Olympus Orbeye (system 1) and the 3D, 960 p VisionSense Iridium (system 2). Near-infrared sensitivity was calculated using signal-to-background ratios (SBRs). In addition, three patients with brain tumors were administered indocyanine-green and imaged with system 1, with two also imaged with system 2 for comparison.
Results
: Systems 1 and 2 detected near-infrared fluorescence from indocyanine green concentrations of >250 μg/L and >31.3 μg/L, respectively. Intraoperatively, system 1 visualized strong near-infrared fluorescence from two, strongly gadoliniumenhancing meningiomas (SBR=2.4, 1.7). The high-resolution, bright images were sufficient for the surgeon to appreciate the underlying anatomy in the near-infrared mode. However, system 1 was not able to visualize fluorescence from a weakly-enhancing intraparenchymal metastasis. In contrast, system 2 successfully visualized both the meningioma and the metastasis but lacked high resolution stereopsis.
Conclusion
: Three-dimensional exoscope systems provide an alternative visualization platform for both standard microsurgery and near-infrared fluorescent guided surgery. However, when tumor fluorescence is weak (i.e., low fluorophore uptake, deep tumors), highly sensitive near-infrared visualization systems may be required.
Keyword
Figure
-

Fig. 1. Excitation and emission profile for system 1 and system 2. A : System 1 is a high-resolution exoscope offering 3-dimensional (3D), 4 K visualization to those wearing circular polarization glasses. It uses light-emitting diodes (LEDs) for illumination. In its near-infrared (NIR) mode, the IR LED turns on, which emits photons of 730–740 nm to excite NIR fluorophores. All returning photons are then collected and filtered by a long-pass filter that blocks photons below 800 nm. A portion of photons <800 nm are let through in order to increase the overall field brightness and allow surgeons to operate in the NIR mode. These photons are then captured by a digital sensor. B : System 2 does not offer stereopsis in its NIR mode but provides enhanced NIR sensitivity. It uses a laser that is tuned to 805 nm to match the peak excitation wavelength of ICG, as seen above. The resulting fluorescence is then filtered through a band-pass filter that allows only photons 820–860 nm to pass. Then, there is an advanced signal processing algorithm which amplifies weaker NIR signal without significant increases in background noise, which enhances NIR signal to background contrast when fluorescence is relatively weaker. Adopted from Cho et al. [8] with permission from the publisher.

Fig. 2. In-vitro analysis of near-infrared (NIR) sensitivity of the two exoscope systems. A : The two exoscope systems were compared directly by imaging serial dilutions of indocyanine green (ICG) from 1.0-2000 μg/L; the results are plotted on a log-scale for the X-axis. System 1 began discriminating the ICG from the control at 250 μg/L, while system 2 was able to detect down to 31.3 μg/L. B : Serial dilution images using system 1. System 1 achieved a signal-to-background ratio (SBR) of 9.7 at the highest concentration of 2000 μg/L. Although image analysis demonstrated the SBR to be 1.9 at 250 μg/L, NIR fluorescence was not visually distinguishable on the screen until the ICG concentration was 500 μg/L. C : Serial dilution images using system 2. System 2 achieved an SBR of 19.2 at the highest concentration of 2000 μg/L. Although image analysis demonstrated the SBR to be 1.5 at 31.3 μg/L, NIR fluorescence was not visually distinguishable on the screen until the ICG concentration was 62.5 μg/L.
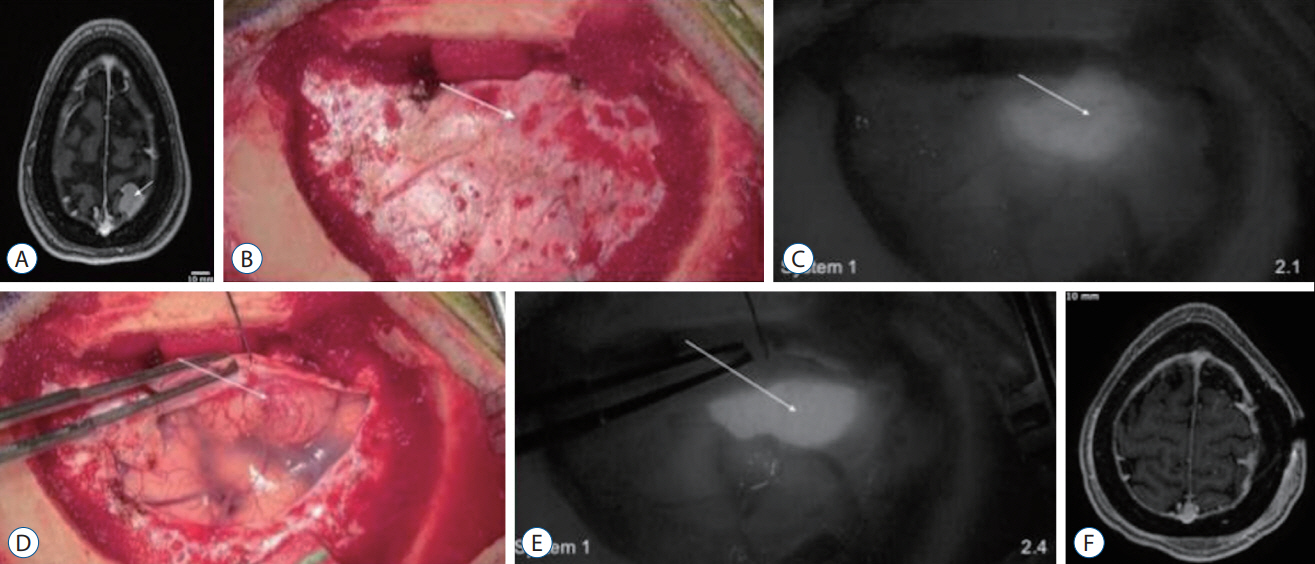
Fig. 3. Demonstration of near-infrared (NIR) fluorescence visualization of a meningioma using system 1 (see Supplementary Video 1). A : Preoperative axial T1 magnetic resonance imaging (MRI) with gadolinium showed a left parietal parasagittal meningioma measuring 17×16×15 mm. The tumor (arrow) enhanced strongly and homogenously with gadolinium. Over the intact dura, white-light imaging (B) did not visualize this superficial tumor (arrow). However, under NIR fluorescence visualization (C), the tumor (arrow) outline was clearly delineated. The tumor demonstrated signal to background ratio of 2.1. With the dura open and the tumor in direct line of sight, the white-light imaging (D) successfully visualized the highly vascular tumor (arrow). Under NIR fluorescence (E), the tumor (arrow) fluoresced even more brightly, with a signal-to-background ratio of 2.4. F : Postoperative axial T1 MRI with gadolinium showed gross total resection of the parietal meningioma without residual neoplasm.

Fig. 4. Demonstration of near-infrared (NIR) fluorescence visualization of a meningioma using system 1 and system 2. A : Preoperative axial T1 magnetic resonance imaging (MRI) with gadolinium showed a right parietal convexity meningioma measuring 46×30×22 mm. The tumor (arrow) enhanced strongly and homogenously with gadolinium. B-E : Over the intact dura, white-light imaging (B) did not visualize this superficial tumor. NIR imaging with system 1 (C) delineated the tumor (arrow) boundaries, with a signal-to-background ratio (SBR) of 1.6. NIR imaging with system 2 in black and white (D) and pseudocolor overlay (E) delineated the tumor more clearly with an SBR of 8.0. F-I : With the dura open and the tumor in direct line of sight, the white-light imaging (F) successfully visualized the tumor (arrow). NIR imaging with system 1 (G) demonstrated high indocyanine green (ICG) accumulation in the tumor, with an NIR SBR of 1.7. System 2 imaging (H and I) demonstrated higher contrast, with an SBR of 10.1. J-M : After devascularization and resection under white-light visualization (J), the tumor specimen was examined under both exoscopes. System 1 (K) again confirmed high ICG accumulation in the tumor, with an SBR of 1.9. System 2 (L and M) also demonstrated very high contrast between the tumor tissue and normal brain, with an SBR of 12.8. N : Postoperative axial T1 MRI with gadolinium showed gross total resection of the convexity meningioma without residual neoplasm.

Fig. 5. Demonstration of near-infrared (NIR) fluorescence visualization in a weakly-enhancing metastasis using system 1 and system 2. A : Preoperative axial T1 magnetic resonance imaging (MRI) with gadolinium showed a cystic, right parietal metastasis. The cystic portion did not enhance with gadolinium and the enhancing portion of the tumor (arrow) did not enhance as intensely as the previous meningiomas. B-E : Over the intact dura, neither white-light imaging (B), system 1 NIR imaging (C), nor system 2 NIR imaging (D and E) could reliably delineate the tumor borders. F-I : With the dura open and over the intact cortex, white-light imaging (F) could not visualize the tumor (arrow). NIR imaging with system 1 (G) also did not detect any NIR fluorescence above that of the surrounding parenchyma (signal-to-background ratio [SBR], 1.15). With system 2 (H and I), NIR fluorescence with an SBR of 2.5 was detected through the cortex in an area consistent with the tumor location. J-M : After exposing the tumor under white-light visualization (J), system 1 NIR visualization showed faint NIR fluorescence in the tumor (K); however, there was not enough signal to distinguish the tumor from the surrounding parenchyma (SBR, 1). With system 2 (L and M), more NIR signal was detected from the tumor, resulting in an SBR of 2.9. N : Postoperative axial T1 MRI with gadolinium showed gross total resection of the parietal metastasis without residual neoplasm.
Reference
-
References
1. Acerbi F, Broggi M, Eoli M, Anghileri E, Cavallo C, Boffano C, et al. Is fluorescein-guided technique able to help in resection of high-grade gliomas? Neurosurg Focus. 36:E5. 2014.
Article2. Belykh E, Miller EJ, Patel AA, Yazdanabadi MI, Martirosyan NL, Yağmurlu K, et al. Diagnostic accuracy of a confocal laser endomicroscope for in vivo differentiation between normal injured and tumor tissue during fluorescein-guided glioma resection: laboratory investigation. World Neurosurg. 115:e337–e348. 2018.3. Chakravarthy V, Sheikh S, Schmidt E, Steinmetz M. Imaging technologies in spine surgery. Neurosurg Clin N Am. 31:93–101. 2020.
Article4. Cho SS, Jeon J, Buch L, Nag S, Nasrallah M, Low PS, et al. Intraoperative near-infrared imaging with receptor-specific versus passive delivery of fluorescent agents in pituitary adenomas. J Neurosurg. 131:1974–1984. 2018.
Article5. Cho SS, Salinas R, De Ravin E, Teng CW, Li C, Abdullah KG, et al. Near-infrared imaging with second-window indocyanine green in newly diagnosed high-grade gliomas predicts gadolinium enhancement on postoperative magnetic resonance imaging. Mol Imaging Biol. 22:1427–1437. 2020.
Article6. Cho SS, Salinas R, Lee JYK. Indocyanine-green for fluorescence-guided surgery of brain tumors: evidence, techniques, and practical experience. Front Surg. 6:11. 2019.
Article7. Cho SS, Teng CW, Ramayya A, Buch L, Hussain J, Harsch J, et al. Surface-registration frameless stereotactic navigation is less accurate during prone surgeries: intraoperative near-infrared visualization using second window indocyanine green offers an adjunct. Mol Imaging Biol. 22:1572–1580. 2020.
Article8. Cho SS, Zeh R, Pierce JT, Salinas R, Singhal S, Lee JYK. Comparison of near-infrared imaging camera systems for intracranial tumor detection. Mol Imaging Biol. 20:213–220. 2018.
Article9. Connally R, Jin D, Piper J. High intensity solid-state UV source for time-gated luminescence microscopy. Cytometry A. 69:1020–1027. 2006.
Article10. DSouza AV, Lin H, Henderson ER, Samkoe KS, Pogue BW. Review of fluorescence guided surgery systems: identification of key performance capabilities beyond indocyanine green imaging. J Biomed Opt. 21:80901. 2016.
Article11. Eljamel MS, Mahboob SO. The effectiveness and cost-effectiveness of intraoperative imaging in high-grade glioma resection; a comparative review of intraoperative ALA, fluorescein, ultrasound and MRI. Photodiagnosis Photodyn Ther. 16:35–43. 2016.
Article12. Fang J, Nakamura H, Maeda H. The EPR effect: unique features of tumor blood vessels for drug delivery, factors involved, and limitations and augmentation of the effect. Adv Drug Deliv Rev. 63:136–151. 2011.
Article13. Hadjipanayis CG, Stummer W. 5-ALA and FDA approval for glioma surgery. J Neurooncol. 141:479–486. 2019.
Article14. Herlan S, Marquardt JS, Hirt B, Tatagiba M, Ebner FH. 3D exoscope system in neurosurgery-comparison of a standard operating microscope with a new 3D exoscope in the cadaver lab. Oper Neurosurg (Hagerstown). 17:518–524. 2019.
Article15. Kaibori M, Matsui K, Ishizaki M, Iida H, Okumura T, Sakaguchi T, et al. Intraoperative detection of superficial liver tumors by fluorescence imaging using indocyanine green and 5-aminolevulinic acid. Anticancer Res. 36:1841–1849. 2016.16. Keating J, Newton A, Venegas O, Nims S, Zeh R, Predina J, et al. Near-infrared intraoperative molecular imaging can locate metastases to the lung. Ann Thorac Surg. 103:390–398. 2017.
Article17. Kwan K, Schneider JR, Du V, Falting L, Boockvar JA, Oren J, et al. Lessons learned using a high-definition 3-dimensional exoscope for spinal surgery. Oper Neurosurg (Hagerstown). 16:619–625. 2019.
Article18. Lee JYK, Cho SS, Stummer W, Tanyi JL, Vahrmeijer AL, Rosenthal E, et al. Review of clinical trials in intraoperative molecular imaging during cancer surgery. J Biomed Opt. 24:1–8. 2019.
Article19. Li C, Buch L, Cho S, Lee JYK. Near-infrared intraoperative molecular imaging with conventional neurosurgical microscope can be improved with narrow band “boost” excitation. Acta Neurochir (Wien). 161:2311–2318. 2019.
Article20. Maeda H. The enhanced permeability and retention (EPR) effect in tumor vasculature: the key role of tumor-selective macromolecular drug targeting. Adv Enzyme Regul. 41:189–207. 2001.
Article21. Murai Y, Sato S, Yui K, Morimoto D, Ozeki T, Yamaguchi M, et al. Preliminary clinical microneurosurgical experience with the 4K3-dimensional microvideoscope (ORBEYE) system for microneurological surgery: observation study. Oper Neurosurg (Hagerstown). 16:707–716. 2019.
Article22. Nishiyama K. From exoscope into the next generation. J Korean Neurosurg Soc. 60:289–293. 2017.
Article23. Pagoto A, Garello F, Marini GM, Tripepi M, Arena F, Bardini P, et al. Novel gastrin-releasing peptide receptor targeted near-infrared fluorescence dye for image-guided surgery of prostate cancer. Mol Imaging Biol. 22:85–93. 2020.
Article24. Ricciardi L, Chaichana KL, Cardia A, Stifano V, Rossini Z, Olivi A, et al. The exoscope in neurosurgery: an innovative “point of view”. A systematic review of the technical, surgical and educational aspects. World Neurosurg. 124:136–144. 2019.
Article25. Ricciardi L, Mattogno PP, Olivi A, Sturiale CL. Exoscope era: next technical and educational step in microneurosurgery. World Neurosurg. 128:371–373. 2019.
Article26. Rossini Z, Cardia A, Milani D, Lasio GB, Fornari M, D’Angelo V. VITOM 3D: preliminary experience in cranial surgery. World Neurosurg. 107:663–668. 2017.
Article27. Sack J, Steinberg JA, Rennert RC, Hatefi D, Pannell JS, Levy M, et al. Initial experience using a high-definition 3-dimensional exoscope system for microneurosurgery. Oper Neurosurg (Hagerstown). 14:395–401. 2018.
Article28. Samkoe KS, Sardar HS, Bates BD, Tselepidakis NN, Gunn JR, Hoffer-Hawlik KA, et al. Preclinical imaging of epidermal growth factor receptor with ABY-029 in soft-tissue sarcoma for fluorescence-guided surgery and tumor detection. J Surg Oncol. 199:1077–1086. 2019.
Article29. Stummer W, Pichlmeier U, Meinel T, Wiestler OD, Zanella F, Reulen HJ, et al. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre phase III trial. Lancet Oncol. 7:392–401. 2006.
Article30. Stummer W, Tonn JC, Goetz C, Ullrich W, Stepp H, Bink A, et al. 5-Aminolevulinic acid-derived tumor fluorescence: the diagnostic accuracy of visible fluorescence qualities as corroborated by spectrometry and histology and postoperative imaging. Neurosurgery. 74:310–320. discussion 319-320. 2014.31. Yasargil MG. Microneurosurgery, Vol 1: Microsurgical Anatomy of the Basal Cisterns and Vessels of the Brain, Diagnostic Studies, General Operative Techniques and Pathological Considerations of the Intracranial Aneurysms. New York: Georg Thieme Verlag Stuttgart;1984.32. Yazaki P, Lwin T, Minnix M, Li L, Sherman A, Molnar J, et al. Improved antibody-guided surgery with a near-infrared dye on a pegylated linker for CEA-positive tumors. J Biomed Opt. 24:1–9. 2019.
Article33. Yu D, Green C, Kasten SJ, Sackllah ME, Armstrong TJ. Effect of alternative video displays on postures, perceived effort, and performance during microsurgery skill tasks. Appl Erg. 53:281–289. 2016.
Article34. Yu D, Sackllah M, Woolley C, Kasten S, Armstrong T. Quantitative posture analysis of 2D, 3D, and optical microscope visualization methods for microsurgery tasks. Work 41 Suppl. 1:1944–1947. 2012.
Article35. Zeh R, Sheikh S, Xia L, Pierce J, Newton A, Predina J, et al. The second window ICG technique demonstrates a broad plateau period for near infrared fluorescence tumor contrast in glioblastoma. PLoS One. 24:e0182034. 2017.
Article36. Zhang DY, Singhal S, Lee JYK. Optical principles of fluorescence-guided brain tumor surgery: a practical primer for the neurosurgeon. Neurosurgery. 85:312–324. 2019.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Utility of Indocyanine Green Fluorescence Imaging in Wound Assessment
- Structure-Inherent Targeting of Near-Infrared Fluorophores for Image-Guided Surgery
- Indocyanine green and near-infrared fluorescenceguided surgery for gastric cancer: a narrative review
- Indocyanine Green-Guided Video-Assisted Thoracoscopic Surgery for Resection of an Ectopic Mediastinal Parathyroid Adenoma
- Real-Time Localization of Parathyroid Glands with Near Infrared Light during Thyroid and Parathyroid Surgery
