Efficacy and tolerability of exclusive enteral nutrition in adult patients with complicated Crohn’s disease
- Sharma S
 1
1 - Gupta A1
- Kedia S1
- Agarwal S1
- Singh N1
- Goyal S1
- Jain S1
- Gupta V1
- Sahu P1
- Vuyyuru SK1
- Kante B1
- Sharma R2
- Panwar R3
- Sahni P3
- Makharia G1
- Ahuja V1
- Affiliations
-
- 1Department of Gastroenterology and Human Nutrition, All India Institute of Medical Sciences, New Delhi, India
- 2Department of Radiodiagnosis, All India Institute of Medical Sciences, New Delhi, India
- 3Department of Gastrointestinal Surgery, All India Institute of Medical Sciences, New Delhi, India
- KMID: 2518685
- DOI: http://doi.org/10.5217/ir.2019.09172
Abstract
- Background/Aims
Exclusive enteral nutrition (EEN), an established modality for pediatric Crohn’s disease (CD) is seldomly utilized in adults. The present study reports the outcome of EEN in adult CD patients at a tertiary care hospital in India.
Methods
This was a retrospective analysis of CD patients who received EEN as a sole modality/adjunct to other treatment. The primary and secondary outcomes changed in Crohn’s Disease Activity Index (CDAI), and clinical response (decline in CDAI > 70), respectively, at 4 and 8 weeks. Subgroup analysis evaluated response across different phenotypes, EEN formulations and prior treatment. Linear mixed effect model was created to assess the predictors of EEN response.
Results
Thirty-one CD patients received EEN over median duration of 4 weeks (range, 2–6 weeks). CDAI showed a significant improvement post EEN at 4 (baseline 290 [260–320] vs. 240 [180–280], P= 0.001) and 8 weeks (baseline 290 [260–320] vs. 186 [160–240], P= 0.001), respectively. The cumulative clinical response rates at 4 and 8 weeks were 37.3% and 80.4% respectively. The clinical response rates at 8 weeks across B1 (n = 4), B2 (n = 18) and B3 (n = 9) phenotypes were 50%, 78.8% and 100% respectively (log-rank test, P= 0.093). The response rates at 8 weeks with polymeric (n = 8) and semi-elemental diet (n = 23) were 75% and 82.6%% respectively (log-rank test, P= 0.49). Baseline CDAI (odds ratio, 1.008; 95% confidence interval, 1.002–1.017; P= 0.046) predicted response to EEN.
Conclusions
EEN was effective in inducing clinical response across different phenotypes of CD. Baseline disease activity remained the most important predictor of clinical response to EEN.
Figure
-
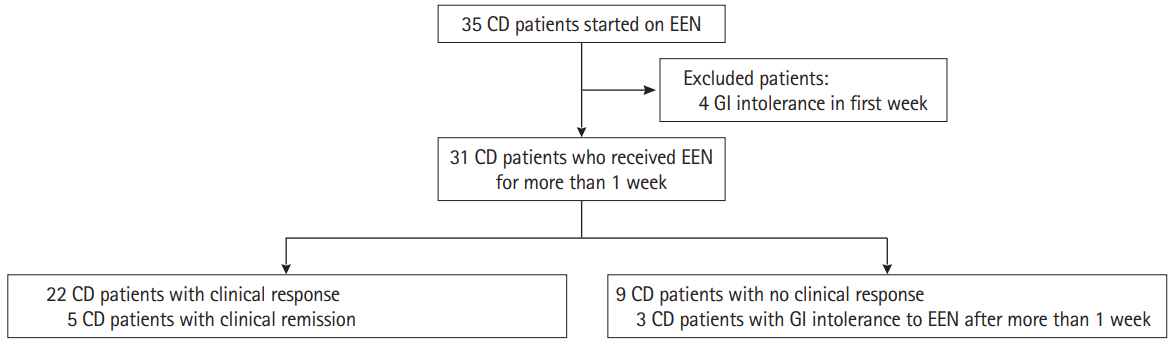
Fig. 1. Flowchart of the patient recruitment in the study. CD, Crohn’s disease; EEN, exclusive enteral nutrition; GI, gastrointestinal.
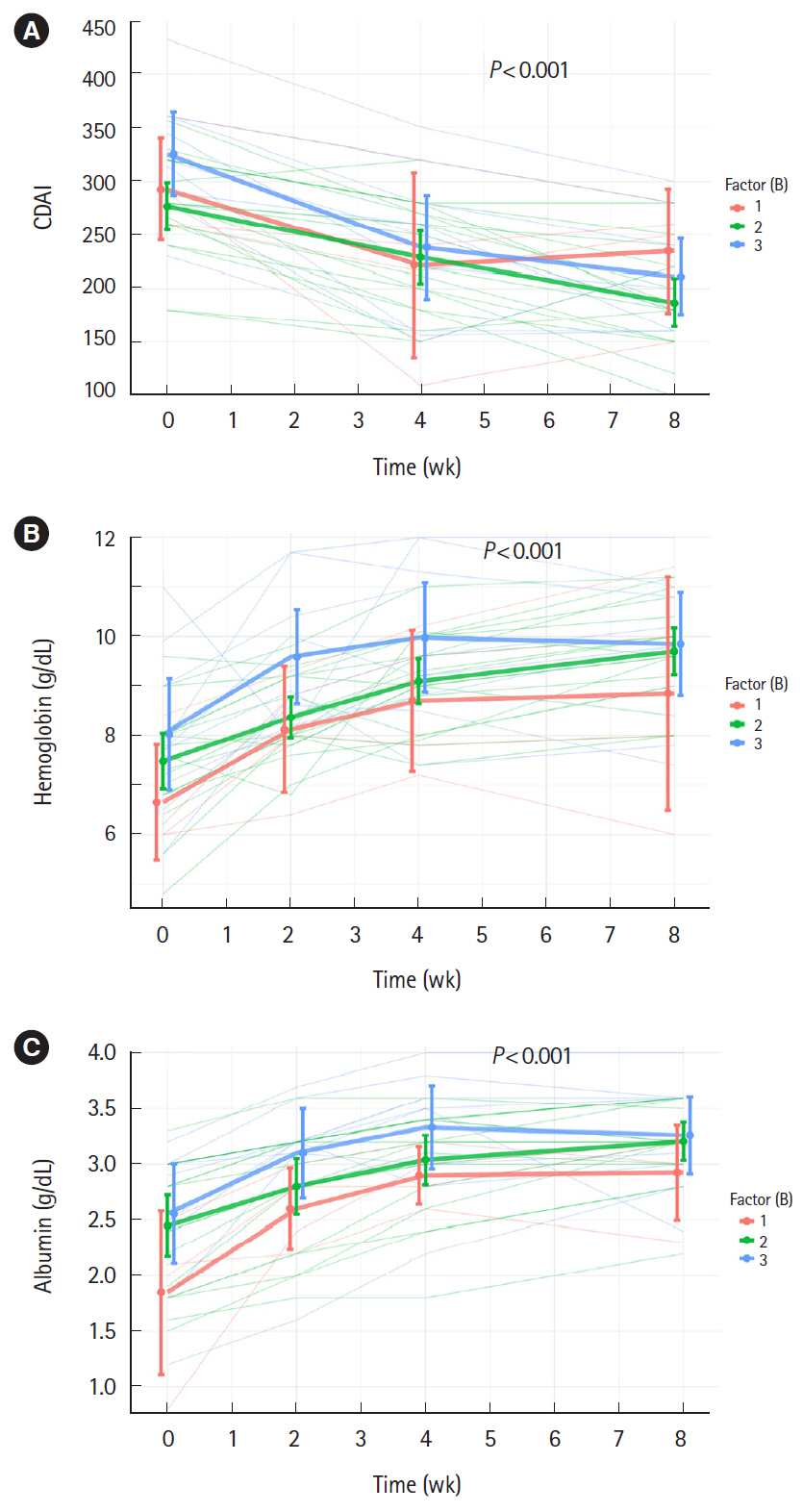
Fig. 2. Profile plots depicting change in Crohn’s Disease Activity Index (CDAI) (A), hemoglobin (B), and serum albumin (C) levels with exclusive enteral nutrition administration across different phenotypes of Crohn’s disease assessed at 4 and 8 weeks respectively.
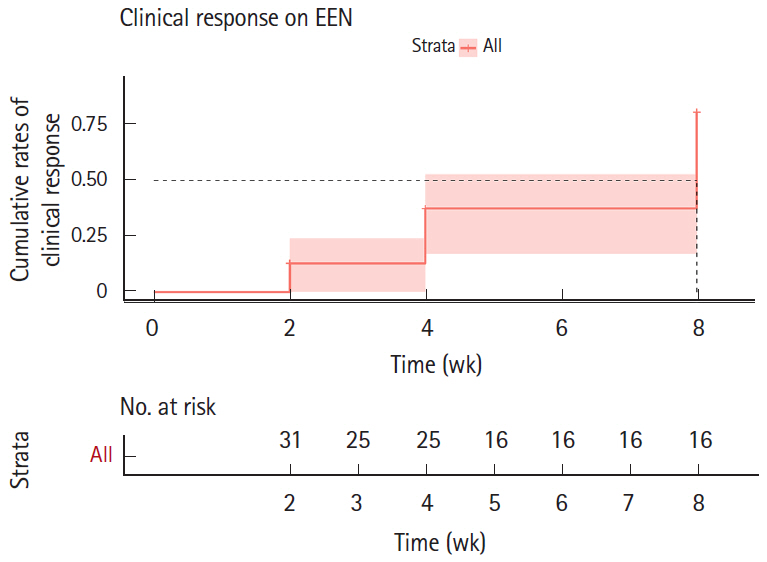
Fig. 3. Kaplan-Meier response plot showing clinical response to exclusive enteral nutrition (EEN). The cumulative clinical response rates to EEN at 4 and 8 weeks were 37.3% and 80.4% respectively.
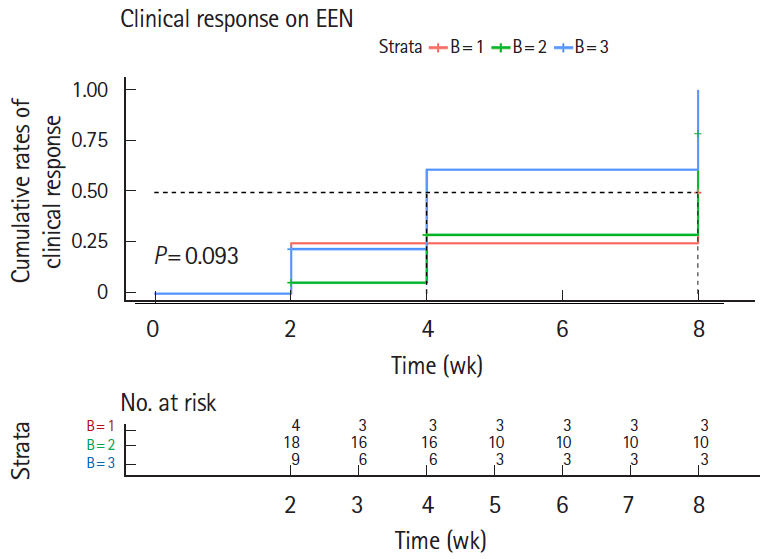
Fig. 4. Kaplan-Meier response plot showing clinical response across different phenotypes of disease. The clinical response rates at 8 weeks in B1 (n=4), B2 (n=18), and B3 (n=9) disease were 50%, 78.8%, and 100% respectively (log-rank test, P=0.093).
Reference
-
1. Torres J, Mehandru S, Colombel JF, Peyrin-Biroulet L. Crohn’s disease. Lancet. 2017; 389:1741–1755.
Article2. Amre DK, D’Souza S, Morgan K, et al. Imbalances in dietary consumption of fatty acids, vegetables, and fruits are associated with risk for Crohn’s disease in children. Am J Gastroenterol. 2007; 102:2016–2025.
Article3. Lee D, Albenberg L, Compher C, et al. Diet in the pathogenesis and treatment of inflammatory bowel diseases. Gastroenterology. 2015; 148:1087–1106.
Article4. Knight-Sepulveda K, Kais S, Santaolalla R, Abreu MT. Diet and inflammatory bowel disease. Gastroenterol Hepatol (N Y). 2015; 11:511–520.5. Sugihara K, Morhardt TL, Kamada N. The role of dietary nutrients in inflammatory bowel disease. Front Immunol. 2019; 9:3183.
Article6. Tomar SK, Kedia S, Upadhyay AD, et al. Impact of dietary beliefs and practices on patients with inflammatory bowel disease: an observational study from India. JGH Open. 2017; 1:15–21.
Article7. Yadav DP, Kedia S, Madhusudhan KS, et al. Body composition in Crohn’s disease and ulcerative colitis: correlation with disease severity and duration. Can J Gastroenterol Hepatol. 2017; 2017:1215035.
Article8. Halkjaer J, Tjønneland A, Thomsen BL, Overvad K, Sørensen TI. Intake of macronutrients as predictors of 5-y changes in waist circumference. Am J Clin Nutr. 2006; 84:789–797.9. Agarwal A, Kedia S, Jain S, et al. High risk of tuberculosis during infliximab therapy despite tuberculosis screening in inflammatory bowel disease patients in India. Intest Res. 2018; 16:588–598.
Article10. Day AS, Lopez RN. Exclusive enteral nutrition in children with Crohn’s disease. World J Gastroenterol. 2015; 21:6809–6816.
Article11. Swaminath A, Feathers A, Ananthakrishnan AN, Falzon L, Li Ferry S. Systematic review with meta-analysis: enteral nutrition therapy for the induction of remission in paediatric Crohn’s disease. Aliment Pharmacol Ther. 2017; 46:645–656.
Article12. Cohen-Dolev N, Sladek M, Hussey S, et al. Differences in outcomes over time with exclusive enteral nutrition compared with steroids in children with mild to moderate Crohn’s disease: results from the GROWTH CD study. J Crohns Colitis. 2018; 12:306–312.
Article13. Connors J, Basseri S, Grant A, et al. Exclusive enteral nutrition therapy in paediatric Crohn’s disease results in long-term avoidance of corticosteroids: results of a propensity-score matched cohort analysis. J Crohns Colitis. 2017; 11:1063–1070.
Article14. Ruemmele FM, Veres G, Kolho KL, et al. Consensus guidelines of ECCO/ESPGHAN on the medical management of pediatric Crohn’s disease. J Crohns Colitis. 2014; 8:1179–1207.15. Forbes A, Escher J, Hébuterne X, et al. ESPEN guideline: clinical nutrition in inflammatory bowel disease. Clin Nutr. 2017; 36:321–347.
Article16. Adamji M, Day AS. An overview of the role of exclusive enteral nutrition for complicated Crohn’s disease. Intest Res. 2019; 17:171–176.
Article17. Li Y, Zuo L, Zhu W, et al. Role of exclusive enteral nutrition in the preoperative optimization of patients with Crohn’s disease following immunosuppressive therapy. Medicine (Baltimore). 2015; 94:e478.
Article18. Wall CL, Gearry RB, Day AS. Treatment of active Crohn’s disease with exclusive and partial enteral nutrition: a pilot study in adults. Inflamm Intest Dis. 2018; 2:219–227.
Article19. Wall CL, Day AS, Gearry RB. Use of exclusive enteral nutrition in adults with Crohn’s disease: a review. World J Gastroenterol. 2013; 19:7652–7660.
Article20. Gomollón F, Dignass A, Annese V, et al. 3rd European evidence-based consensus on the diagnosis and management of Crohn’s disease 2016. Part 1: diagnosis and medical management. j crohns colitis. 2017; 11:3–25.
Article21. Best WR, Becktel JM, Singleton JW, Kern F Jr. Development of a Crohn’s disease activity index. National Cooperative Crohn’s Disease Study. Gastroenterology. 1976; 70:439–444.22. Satsangi J, Silverberg MS, Vermeire S, Colombel JF. The Montreal classification of inflammatory bowel disease: controversies, consensus, and implications. Gut. 2006; 55:749–753.
Article23. Peyrin-Biroulet L, Loftus EV Jr, Colombel JF, Sandborn WJ. The natural history of adult Crohn’s disease in population-based cohorts. Am J Gastroenterol. 2010; 105:289–297.
Article24. Sandborn WJ, Feagan BG, Hanauer SB, et al. A review of activity indices and efficacy endpoints for clinical trials of medical therapy in adults with Crohn’s disease. Gastroenterology. 2002; 122:512–530.
Article25. Voitk AJ, Echave V, Feller JH, Brown RA, Gurd FN. Experience with elemental diet in the treatment of inflammatory bowel disease. Is this primary therapy? Arch Surg. 1973; 107:329–333.
Article26. Borrelli O, Cordischi L, Cirulli M, et al. Polymeric diet alone versus corticosteroids in the treatment of active pediatric Crohn’s disease: a randomized controlled open-label trial. Clin Gastroenterol Hepatol. 2006; 4:744–753.
Article27. Yu Y, Chen KC, Chen J. Exclusive enteral nutrition versus corticosteroids for treatment of pediatric Crohn’s disease: a meta-analysis. World J Pediatr. 2019; 15:26–36.
Article28. Narula N, Dhillon A, Zhang D, Sherlock ME, Tondeur M, Zachos M. Enteral nutritional therapy for induction of remission in Crohn’s disease. Cochrane Database Syst Rev. 2018; 4–CD000542.
Article29. Yang Q, Gao X, Chen H, et al. Efficacy of exclusive enteral nutrition in complicated Crohn’s disease. Scand J Gastroenterol. 2017; 52:995–1001.
Article30. Hu D, Ren J, Wang G, et al. Exclusive enteral nutritional therapy can relieve inflammatory bowel stricture in Crohn’s disease. J Clin Gastroenterol. 2014; 48:790–795.
Article31. Wu XL, Chen RP, Tao LP, Wu JS, Chen XR, Chen WC. Infliximab combined with enteral nutrition for managing Crohn’s disease complicated with intestinal fistulas. Gastroenterol Res Pract. 2016; 2016:5947926.
Article32. Hisamatsu T, Kunisaki R, Nakamura S, et al. Effect of elemental diet combined with infliximab dose escalation in patients with Crohn’s disease with loss of response to infliximab: CERISIER trial. Intest Res. 2018; 16:494–498.
Article33. Hirai F, Takeda T, Takada Y, et al. Efficacy of enteral nutrition in patients with Crohn’s disease on maintenance anti-TNF-alpha antibody therapy: a meta-analysis. J Gastroenterol. 2020; 55:133–141.
Article34. Yamamoto T, Nakahigashi M, Umegae S, Kitagawa T, Matsumoto K. Impact of elemental diet on mucosal inflammation in patients with active Crohn’s disease: cytokine production and endoscopic and histological findings. Inflamm Bowel Dis. 2005; 11:580–588.
Article35. Afzal NA, Davies S, Paintin M, et al. Colonic Crohn’s disease in children does not respond well to treatment with enteral nutrition if the ileum is not involved. Dig Dis Sci. 2005; 50:1471–1475.
Article36. Buchanan E, Gaunt WW, Cardigan T, Garrick V, McGrogan P, Russell RK. The use of exclusive enteral nutrition for induction of remission in children with Crohn’s disease demonstrates that disease phenotype does not influence clinical remission. Aliment Pharmacol Ther. 2009; 30:501–507.
Article37. Liu J, Andrews JM, Sammour T, et al. Benefits of exclusive enteral nutrition in adults with complex active Crohn’s disease: a case series of 13 consecutive patients. Crohns Colitis 360. 2019; 1–otz044.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- An overview of the role of exclusive enteral nutrition for complicated Crohn's disease
- Exclusive Enteral Nutrition for the Treatment of Pediatric Crohn’s Disease: The Patient Perspective
- Therapeutic Efficacy of Exclusive Enteral Nutrition with Specific Polymeric Diet in Pediatric Crohn's Disease
- Advantages of enteral nutrition
- Nutritional approach as therapeutic manipulation in inflammatory bowel disease
