Importance of High-Frequency Vestibular Function in the Prognosis of Bilateral Vestibulopathy
- Affiliations
-
- 1Department of Otorhinolaryngology, Yonsei University College of Medicine, Seoul, Korea
- KMID: 2515432
- DOI: http://doi.org/10.21053/ceo.2020.01739
Abstract
Objectives
. The aim of this study was to investigate whether preserved vestibular function in the high-frequency range influences the prognosis of patients with bilateral vestibulopathy (BVP) after vestibular rehabilitation.
Methods
. Twenty-four patients followed up with vestibular rehabilitation were recruited. The enrolled patients were divided into two groups according to the preservation of the high-frequency vestibulo-ocular reflex (VOR) based on the video head impulse test (vHIT). The results of computerized dynamic posturography and the Dizziness Handicap Inventory (DHI) survey collected at baseline and at the 6-month follow-up after vestibular rehabilitation therapy were analyzed.
Results
. Both groups showed significantly increased composite and DHI scores after follow-up with vestibular rehabilitation. The group with preserved high-frequency VOR showed a better composite score (p=0.064) and vestibular score (p= 0.008) than the group with lost high-frequency VOR at the 6-month follow up. The DHI score significantly decreased only in the group with lost high-frequency VOR (p=0.047). Among the three vestibular function tests (caloric test, rotary chair test, and vHIT) used to diagnose BVP, only vHIT showed a significant correlation (p=0.015) with a favorable prognosis (composite score ≥70).
Conclusion
. Better treatment outcomes are likely in patients with BVP with preserved vestibular function in response to high-frequency stimulation, as measured by the vHIT.
Keyword
Figure
-
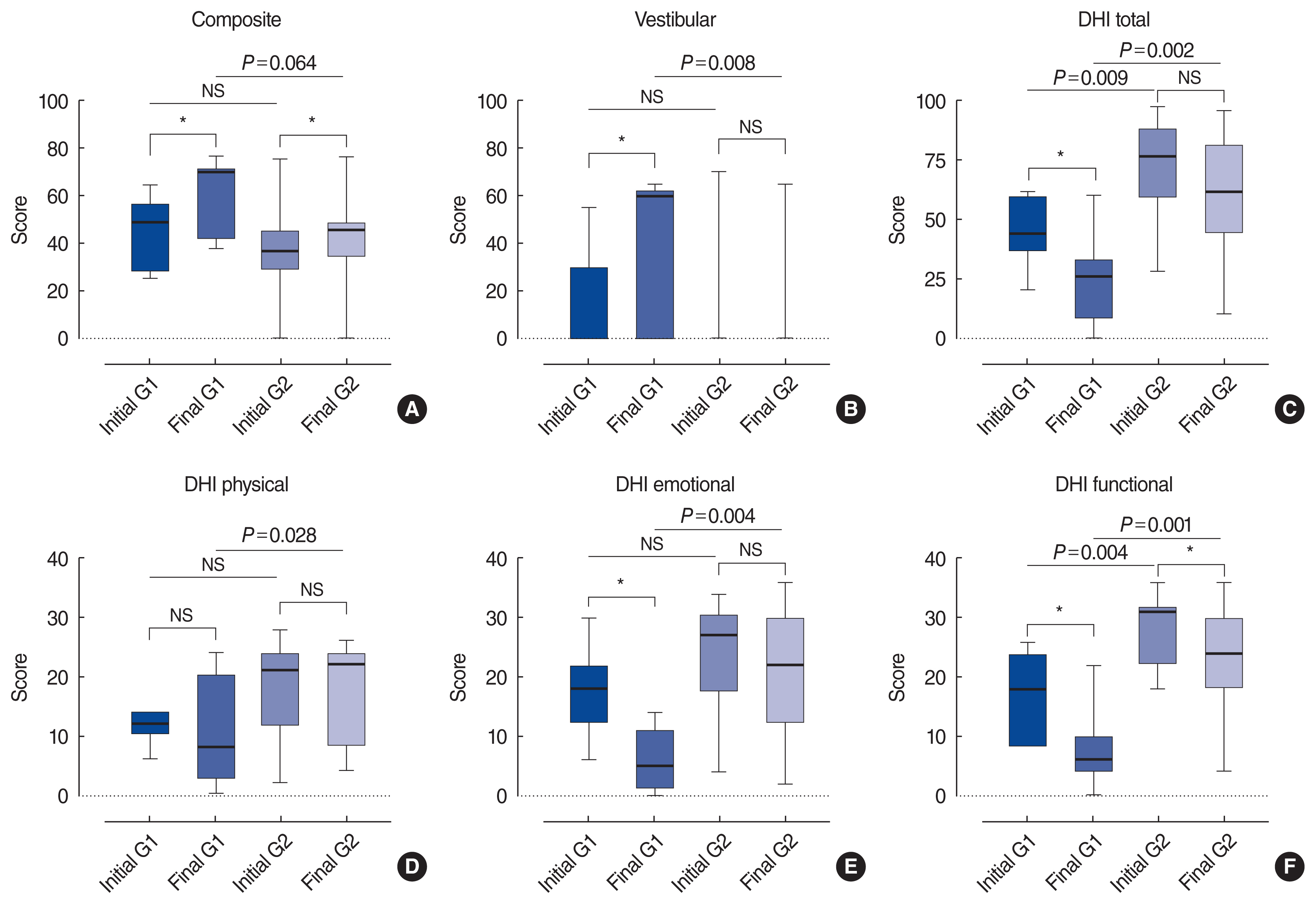
Fig. 1 Changes in subjective symptoms and objective parameters of balance function after rehabilitation. A simple boxplot of the computerized dynamic posturography and Dizziness Handicap Inventory (DHI) scores for bilateral vestibulopathy patients at baseline and follow-up. G1 (group 1, video head impulse test [vHIT] gain in the lateral semicircular canal [LSCC] ≥0.6 in one or both ears) patients showed a better outcome than G2 (group 2, vHIT gain in the LSCC <0.6 in both ears) patients. (A) Composite score, (B) vestibular score, (C) DHI total score, (D) DHI physical score, (E) DHI emotional score, and (F) DHI functional score. The line in the middle is the median. The top and bottom box lines show the first and third quartiles, respectively. The whiskers show the maximum and minimum values. NS, not significant. *P<0.05.
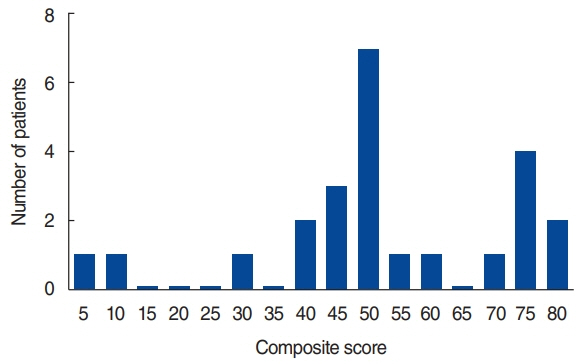
Fig. 2 Distribution of patients according to the final composite score after vestibular rehabilitation. The cumulative graph of the final composite score showed a double peak at 45–50 and 70–75.
Reference
-
1. Zingler VC, Weintz E, Jahn K, Mike A, Huppert D, Rettinger N, et al. Follow-up of vestibular function in bilateral vestibulopathy. J Neurol Neurosurg Psychiatry. 2008; Mar. 79(3):284–8.
Article2. Minor LB, Goldberg JM. Influence of static head position on the horizontal nystagmus evoked by caloric, rotational and optokinetic stimulation in the squirrel monkey. Exp Brain Res. 1990; 82(1):1–13.
Article3. Alhabib SF, Saliba I. Video head impulse test: a review of the literature. Eur Arch Otorhinolaryngol. 2017; Mar. 274(3):1215–22.
Article4. Halmagyi GM, Chen L, MacDougall HG, Weber KP, McGarvie LA, Curthoys IS. The video head impulse test. Front Neurol. 2017; Jun. 9. 8:258.
Article5. Gillespie MB, Minor LB. Prognosis in bilateral vestibular hypofunction. Laryngoscope. 1999; Jan. 109(1):35–41.
Article6. Lacour M, Bernard-Demanze L. Interaction between vestibular compensation mechanisms and vestibular rehabilitation therapy: 10 recommendations for optimal functional recovery. Front Neurol. 2015; Jan. 5:285.
Article7. Minor LB. Gentamicin-induced bilateral vestibular hypofunction. JAMA. 1998; Feb. 279(7):541–4.
Article8. Krebs DE, Gill-Body KM, Riley PO, Parker SW. Double-blind, placebo-controlled trial of rehabilitation for bilateral vestibular hypofunction: preliminary report. Otolaryngol Head Neck Surg. 1993; Oct. 109(4):735–41.
Article9. Porciuncula F, Johnson CC, Glickman LB. The effect of vestibular rehabilitation on adults with bilateral vestibular hypofunction: a systematic review. J Vestib Res. 2012; 22(5–6):283–98.
Article10. Schubert MC, Migliaccio AA, Clendaniel RA, Allak A, Carey JP. Mechanism of dynamic visual acuity recovery with vestibular rehabilitation. Arch Phys Med Rehabil. 2008; Mar. 89(3):500–7.
Article11. Herssens N, Verbecque E, McCrum C, Meijer K, van de Berg R, Saeys W, et al. A systematic review on balance performance in patients with bilateral vestibulopathy. Phys Ther. 2020; Aug. 100(9):1582–94.
Article12. Strupp M, Kim JS, Murofushi T, Straumann D, Jen JC, Rosengren SM, et al. Bilateral vestibulopathy: diagnostic criteria consensus document of the classification Committee of the Barany Society. J Vestib Res. 2017; 27(4):177–89.13. Jeong J, Jung J, Lee JM, Suh MJ, Kwak SH, Kim SH. Effects of saccular function on recovery of subjective dizziness after vestibular rehabilitation. Otol Neurotol. 2017; Aug. 38(7):1017–23.
Article14. Jung J, Suh MJ, Kim SH. Discrepancies between video head impulse and caloric tests in patients with enlarged vestibular aqueduct. Laryngoscope. 2017; Apr. 127(4):921–6.
Article15. Oda DT, Gananca CF. Computerized dynamic posturography in the assessment of body balance in individuals with vestibular dysfunction. Audiol Commun Res. 2015; 20(2):89–95.16. Gera G, Freeman DL, Blackinton MT, Horak FB, King L. Identification of balance deficits in people with Parkinson disease: is the sensory organization test enough? Int J Phys Med Rehabil. 2016; Feb. 4(1):322.
Article17. Demer JL, Oas JG, Baloh RW. Visual-vestibular interaction in humans during active and passive, vertical head movement. J Vestib Res. 1993; Summer. 3(2):101–14.18. Meyer CH, Lasker AG, Robinson DA. The upper limit of human smooth pursuit velocity. Vision Res. 1985; 25(4):561–3.
Article19. Rey-Martinez J, Batuecas-Caletrio A, Matino E, Trinidad-Ruiz G, Altuna X, Perez-Fernandez N. Mathematical methods for measuring the visually enhanced vestibulo-ocular reflex and preliminary results from healthy subjects and patient groups. Front Neurol. 2018; Feb. 9:69.
Article20. Roy FD, Tomlinson RD. Characterization of the vestibulo-ocular reflex evoked by high-velocity movements. Laryngoscope. 2004; Jul. 114(7):1190–3.
Article21. Grossman GE, Leigh RJ, Abel LA, Lanska DJ, Thurston SE. Frequency and velocity of rotational head perturbations during locomotion. Exp Brain Res. 1988; 70(3):470–6.
Article22. Hirasaki E, Moore ST, Raphan T, Cohen B. Effects of walking velocity on vertical head and body movements during locomotion. Exp Brain Res. 1999; Jul. 127(2):117–30.
Article23. Herdman SJ, Schubert MC, Tusa RJ. Role of central preprogramming in dynamic visual acuity with vestibular loss. Arch Otolaryngol Head Neck Surg. 2001; Oct. 127(10):1205–10.
Article24. Heimbrand S, Bronstein AM, Gresty MA, Faldon ME. Optically induced plasticity of the cervico-ocular reflex in patients with bilateral absence of vestibular function. Exp Brain Res. 1996; Dec. 112(3):372–80.
Article
